Download
1 / 33
340 likes | 404 Views
MMPI-2. William P. Wattles, Ph.D. Francis Marion University. MMPI-2 with Adolescents. Should not be used with people less than 18. MMPI-2 with Older Adults. Higher scores on: 1, 2, 3, 0 Lower scores on: 4, 9 MMPI-2 generally valid with older adults. Studies with older adults.

E N D
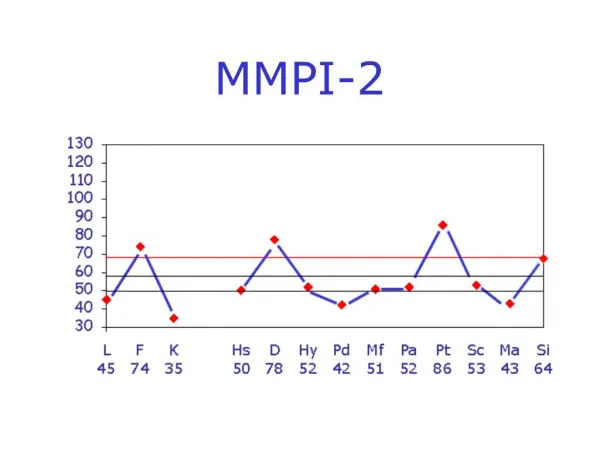
MMPI-2 William P. Wattles, Ph.D. Francis Marion University
MMPI-2 with Adolescents • Should not be used with people less than 18
MMPI-2 with Older Adults • Higher scores on: • 1, 2, 3, 0 • Lower scores on: • 4, 9 • MMPI-2 generally valid with older adults
Studies with older adults • Most studies cross-sectional • Cohort factors • One longitudinal study found similar results • Differences do not suggest pathology but genuine concerns about health. • Age-related changes in physical health
Cohort Effects • Patterns of disease frequency due to an exposure occurring to a group of people at about the same time in their lives
MMPI-2 with Ethnic Minorities • Assessing MMPI-2 and minorities • Any difference = bias • Assess Validity
Data on African-Americans • Slightly higher scores on scales 8 & 9. • Not seen when matched for demographics, ses • Differences tend to be associated with relevant extratest characteristics.
Explanation for differences • Accurate measurement of different personality traits. • Social desirability • Role conflicts • Modesty expectations • Language/experience
MMPI-2 with Ethnic Minorities • No consistent differences across all populations • Moderator variables such as education, income, age, and type of pathology explain most differences.
MMPI-2 with Hispanics • Differences between groups relatively small and not statistically or clinically significant. • Language and reading obviously an issue.
Medical Patients • Large Mayo clinic study suggests that medical problems alone do not result in elevated profiles.
Screening for Substance Abuse • Elevated Scale 4 • Mac Andrews Scale • AAS • APS • Beware false negatives
MMPI-2 and employment screening • Screen for psychopathology • Limited to sensitive occupations • Air traffic controller • Police officer • Nuclear power plant operator • Predict quality of job performance • Negative work attitude scale interesting • MMPI-2 Not recommended
MMPI-2 and employment screening • Applicants usually defensive. • Invalid profile for defensiveness should not be cause to disqualify. • Thus, scores above 65 meaningful • 60-65 may indicate problems.
Report writing • Interpretive strategy • Use MMPI-2 to generate hypotheses • Not all interpretive data applies to each subject • MMPI-2 deal in probabilities • Blind interpretation problematic
Report writing • Test-taking attitude • Missing items may indicate indecisiveness, ambivalence • Long test times can mean indecisiveness, confusion • Qualitative analysis of behavior • Upset • Atypical difficulties
Report writing • Test-taking attitude • Yea-saying (TRIN) • L scale naïve, global denial • K scale defensive, self-critical
Report Writing • Adjustment Level • Psychological comfort, overall elevation • Scores above 65 suggest discomfort. • Welsh’s Anxiety (A) • Ego Strength (ES)
Characteristic Functioning • Symptoms • Major needs • Dependency, achievement • Perceptions • View of others and optimism • Reactions to stress • Coping style and effectiveness • Self-concept
Characteristic Functioning • Sexual orientation • Emotional control • Interpersonal relationships • Psychological resources
Dynamics and Etiology • Higher order inferences about underlying dynamics and cause
Diagnostic Impressions • MMPI-2 can be a tool in settling on a diagnosis if required for insurance etc. • Diagnosis can be in the form of a symptom description.
Treatment Implications. • A primary goal of assessment is to make treatment recommendations. • To treat or not • Type of treatment • Prognosis • Receptiveness to treatment • Motivation
Somatic Symptom and Related Disorders • Individuals with these disorders primarily present in medical rather than mental health settings. • All of these disorders involve a prominent focus on somatic concerns.
Somatic Symptom Disorder • Persistent somatic symptoms • Preoccupation with physical symptoms.
Somatization is a tendency to experience and communicate psychological distress in the form of somatic symptoms and to seek medical help for them. More commonly expressed, it is the generation of physical symptoms of a psychiatric condition such as anxiety.
Somatization occurs when psychological concerns are converted into physical symptoms. Though they have no underlying physical cause, somatic symptoms, such as pain or nausea, are very real and have not been invented by the person experiencing them.
Fibromyalgia • a fibromyalgia diagnosis can be made if a person has had widespread pain for more than three months — with no underlying medical condition that could cause the pain.
Chronic fatigue syndrome • Chronic fatigue syndrome (CFS) is a complicated disorder characterized by extreme fatigue that can't be explained by any underlying medical condition. The fatigue may worsen with physical or mental activity, but doesn't improve with rest.
Irritable bowel syndrome • Irritable bowel syndrome (IBS) is one of the most common diagnoses made by gastroenterologists and primary care providers alike, and yet the underlying causes of IBS are poorly understood. • In diagnosing irritable bowel syndrome, your symptoms and their severity are only part of the picture. Other causes need to be ruled out.