Download
1 / 27
290 likes | 523 Views
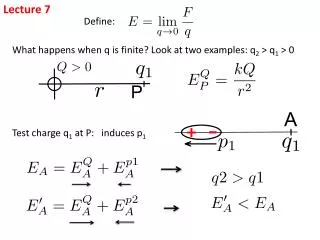
Lecture 7. The Shoulder. Anatomy Review The shoulder is difficult to assess because of the many structure located in a small area There are a number of different joints and the shoulder may be a site of referred pain. Glenohumeral Joint Mulit-axial ball and socket synovial joint

E N D
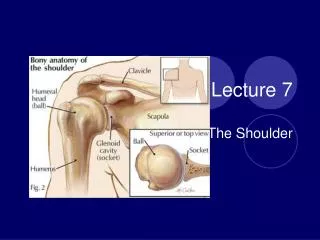
Lecture 7 The Shoulder
Anatomy Review • The shoulder is difficult to assess because of the many structure located in a small area • There are a number of different joints and the shoulder may be a site of referred pain
Glenohumeral Joint • Mulit-axial ball and socket synovial joint • Depends on muscle rather than ligaments for support • Has a labrum – or a ring of fibrocartilage that surrounds and deepens the glenoid cavity
Resting position • 55 degrees of abduction • 30 degrees of cross extension • The humerus sits in the upper part of the glenoid cavity with contraction of the rotator cuff muscles it is pulled down into the lower wider part – allowing for full abduction
Ligaments of the GH • Superior, middle and inferior glenohumeral ligaments • Z – shaped band across the front of the GH joint • Weak and easily stretched
AC Joint • Irregular diarthrodial joint • limited motion in all three planes • Augments the ROM of the humerus • Resting position • arm by side
Ligaments of the AC • Acromioclavicular • Coracoclavicular • Both function to hold clavicle down
Sternoclavicular Joint • Along with the AC joint the SC joint enables the humerus to move through a full 180 degrees of abduction • Saddle shaped – synovial joint • Medial end of clavicle and manubrium of the sternum and cartilage of the first rib • Disc between the two ends of joint • ROM include elevation, depression, protraction and retraction (rotation)
Scapulothoracic joint • Not a true joint • Functions as an integral part of the shoulder complex - important in stabilization of shoulder and facilitates movement • Body of scapula and muscles covering the posterior wall of the chest form this pseudo joint
Scapulohumeral rhythm • the coordination of the scapular and humeral movements • this enables much greater ROM of the shoulder • If arm elevated past 30 abduction or 45-60 of flexion the scapula rotates , contributing 1/3 of total rotational movement of the humerus
Roughly 2-1 rotation of humerus to scapula • Hiking of the shoulder • reverse scapulohumeral rhythm – scapula moves more than the humerous
Winging of the scapula • winging of the medial border of the scapula • indicative of injury or weakness of the serratus anterior muscle or the long thoracic nerve • have athlete stand at wall and do a push up to see winging of scapula • ROM end feels
ROM of shoulder • LR/MR (ER/IR) Ext/Flex, Abd/add, cross flex/cross ext, ( hor-abd/hor-add) circumduction • Muscles ?
AC Distraction / Compression Test • AC joint • apply downward traction (distraction) on the upper extremity , this will lead to downward movement of acromion away from clavicle if AC is unstable • positive test - will produce pain and joint movement • AC Compression • Horizontal adduction of humerus across the chest compresses the AC joint and will lead to pain if injured • positive test - will produce pain
Load and shift • GH joint instability • Athlete sitting or supine • Press humerus into the glenoid cavity (the load) • Move humeral head Ant/post noting the amount of translation (shift) • Positive test – more movement( instability) • Normal is about 25% of humeral head diameter • http://www.youtube.com/watch?v=uhBWu9TJsJ8&feature=related • http://www.youtube.com/watch?v=WnlpkEWXIiU
Apprehension / Crank test ( anterior instability) GH joint • Examiner passively abducts the arm to 90 degrees and LR athletes shoulder slowly • positive test - is indicated by the feeling or look of apprehension of the athlete • Athlete will likely resist further movement • Do this test very slowly as this is the position of most dislocations • http://www.youtube.com/watch?v=qKqJRrms4u8&feature=channel
Sulcus Sign (Inferior instability) GH joint • Examiner grasps athletes forearm below elbow and pulls down (distally) • The arm is in a neutral position with no rotation and slight abduction (10 – 20 degrees) • Positive test- Presence of a sulcus at the top of the shoulder is a positive sign of inferior instability • If athlete has an inferior instability – usually multidirectional instability as well • http://www.youtube.com/watch?v=lsaOqetQZpw
Speed’s Test Biceps tendon • Athletes arm is straight out in a flexed position with the palm up (supinated) • Examiner then pushed down on the forearm (pushing into extension) • Positive test - is pain and weakness in the anterior part of the shoulder (bicepital groove) • Indicative of biceps tendon injury (long head) • http://www.youtube.com/watch?v=N00gA4Pvsbw&feature=channel
Empty can • Supraspinatus • Athlete stands with arm out to side (approx 45 degrees cross extension) • Thumb is pointed down (arm internally rotated) • Examiner pushes down on the forearm • Positive test -is pain and weakness • Indicative of a supraspinatus tendinitis or strain • http://www.youtube.com/watch?v=qjHOqydDhxo
Drop Arm Rotator cuff • Examiner passively abducts the athletes arm to 90 degrees • Athlete tries to hold it there and then slowly lower arm to side • Positive test -occurs when athlete can not lower arm slowly and with out pain • Indicative of a tear in the Rotator cuff complex • http://www.youtube.com/watch?v=taVMaab9e8c&feature=related
Hawkin’s Test • Impinges supraspinatus muscle, Teres Minor muscle, and Infraspinatus muscle • Hawk trainers hold their arm in the starting position of this test • Shoulder forward flexed to 90 degrees • Elbow flexed to 90 degrees • Examiner grasps patients elbow with one hand and their wrist with the other • Examiner passively internally rotates the shoulder • Positive sign – pain – shoulder impingement
Costoclavicular syndrome test • Test for thoracic outlet syndrome • Examiner palpates the radial pulse then draws athletes shoulder down and back while athlete hyperextends their neck • Positive test - is a diminishing or absence of radial pulse • Subclavian artery is being blocked by costolclavicular structures of the shoulder
Adson Maneuver • Test for thoracic outlet syndrome • Examiner palpates radial pulse • Athlete rotates head toward affected shoulder ( keeps head extended) , while examiner LR and extends shoulder • Athlete takes a deep breath and holds • Positive test - if radial pulse diminishes or is absent, then subclavian artery is being blocked by anterior and middle scalene muscles
Sport Specific Functional Tests • All functional patterns should be fluid and painfree • throwing • swimming strokes • overhead serves...