Download

1 / 50
510 likes | 798 Views
HDL Cholesterol No Longer Is Good Cholesterol: Emerging Genetic Theories. Sunita Dodani & Janice S Dorman University of Pittsburgh (Study proposal). Presentation Overview. Study background & significance Basic description & function of lipids, lipoproteins and apoproteins

E N D
HDL Cholesterol No Longer Is Good Cholesterol: Emerging Genetic Theories Sunita Dodani & Janice S Dorman University of Pittsburgh (Study proposal)
Presentation Overview • Study background & significance • Basic description & function of lipids, lipoproteins and apoproteins • HDL & apoprotein A-1 • New theories of LDL & HDL role in atherosclerosis • Concept of dysfunctional HDL • Hypothesized causes of dysfunctionalHDL • Study Rationale • Study objectives • Study Design & Methods
Study background & significance • Fats are triacylglycerols containing saturated fatty acids- solid at room temp - usually from animal source (however, coconut & palm oil are saturated). • Oils are triacylglycerols containing mono- or polyunsaturated fatty acids - liquid at room temp - usually from plant sources (however, fish oils are polyunsaturated). • Phospholipids are triacylglycerols that have a FA replaced with a phosphate linked FA group. • The major dietary sterol is cholesterol.
Functions Of Lipids • Major components of cell membranes. • Required to solubilise fat soluble vitamins • Biosynthetic precursors (e.g. steroid hormones from cholesterol) • Protection (e.g. kidneys are shielded with fat in fed state) • Insulation
Lipid transport in the circulation Proteins (apoproteins) Cholesterol Non polar lipids in core (TAG and cholesterol esters) Lipids are insoluble in plasma. In order to be transported they are combined with specific proteins to form lipoproteins
Lipoproteins • Particles found in plasma that transport lipids including cholesterol • Spherical particles with a hydrophobic core (TG and esterified cholesterol) • Apolipoproteins on the surface • large: apoB (b-48 and B-100) atherogenic • smaller: apoA-I, apoC-II, apoE • Classified on the basis of density (NMR spectroscopy) and electrophoretic mobility (VLDL; LDL; IDL;HDL; Lp-a)
Five classes of lipoprotein(all contain characteristic amounts TAG, cholesterol, cholesterol esters, phospholipids and Apoproteins – NMR Spectroscopy) Increasing density
Atherogenic Particles MEASUREMENTS: Apolipoprotein B Non-HDL-C VLDL IDL VLDLR Small,denseLDL LDL TG-rich lipoproteins
The Apolipoproteins • Major components of lipoproteins • Often referred to as aproteins • Classified by alphabetical designation (A thru E) • The use of roman numeral suffix describes the order in which the Apolipoproteins emerge from a chromatographic column • Responsible for recognition of particle by receptors
Apoproteins of human lipoproteins • A-I (28,300)- principal protein in HDL • 90 –120 mg% in plasma • A-II (8,700) – occurs as dimer mainly in HDL • 30 – 50 mg %; enhances hepatic lipase activity • B-48 (240,000) – found only in chylomicrons • <5 mg %; derived from apo-B-100 gene by RNA editing; lacks the LDL receptor-binding domain of apo-B-100 • B-100 (500,000) – principal protein in LDL • 80 –100 mg %; binds to LDL receptor (Circulation. 2004 Jun 15;109(23 Suppl):III2-7)
Apoproteins of human lipoproteins • C-I (7,000) – found in chylomicrons, VLDL, HDL • 4 – 7 mg %; may also activate LCAT • C-II (8,800) - found in chylomicrons, VLDL, HDL • 3 – 8 mg %; activates lipoprotein lipase • C-III (8,800) - found in chylomicrons, VLDL, IDL, HDL • 8 15 mg %; inhibits lipoprotein lipase • D (32,500) - found in HDL • 8 – 10 mg %; also called cholesterol ester transfer protein (CETP) • E (34,100) - found in chylomicrons, VLDL, IDL HDL • 3 – 6 mg %; binds to LDL receptor • H (50,000) – found in chylomicrons; also known as b-2-glycoprotein I (involved in TG metabolism)
Chylomicrons Major lipoprotein classes • Formed through extrusion of resynthesized triglycerides from the mucosal cells into the intestinal lacteals • Flow through the thoracic ducts into the subclavian veins • Degraded to remnants by the action of lipoprotein lipase (LpL) which is located on capillary endothelial cell surface • Remnants are taken up by liver parenchymal cells
Major lipoprotein classes • VLDL • density >1.006 • diameter 30 - 80nm • endogenous triglycerides • apoB-100, apoE, apoC-II/C-III • prebeta in electrophoresis • formed in the liver as nascent VLDL (contains only triglycerides, apoE and apoB)
B100 VLDL Tissues Lipoprotein lipase Capillary wall (endothelial surface) This animation shows how VLDL are metabolised once they enter the circulation from the liver B100 LDL E CII Some LDL taken up by liver (LDL receptors) Having lost TAG to tissues LDL contains a large proportion of cholesterol/cholesterol esters Some LDL taken up by other tissues (LDL receptors). LDL delivers cholesterol and TAG to the extra hepatic tissues. E CII HDL
LDL membrane receptor • Found in clathrin coated pits (endocytosis) • After endocytosis the receptor is recycled whilst the LDL is degraded to releasing lipid cargo. Cholesterol uptake down regulates the cells own production of cholesterol and down regulates LDL receptor synthesis • Mutations in LDL receptors causes increased plasma LDL levels (i.e. increased cholesterol levels). This accelerates progress of atherosclerosis (Familial hyperlipedimias). • The cholesterol in LDL is often called “bad cholesterol”.
Production of Small Dense LDL Although size (& lipid content) changes, there is always 1 molecule apo B protein / particle Lipoprotein receptors B B B Oxidation & modification B Lipase TG CE • (CETP) • Lipids • transferred VLDL remnants IDL LDL VLDL large dense 1 2 3
B B CE CE Tg Tg Relative Atherogenicity of Large and Small LDL Particles
High density lipoprotiens • Act as a reservoir for apoproteins which can be donated or received from other lipoproteins. • Also play a vital role in scavenging “used” cholesterol (reverse cholesterol transport): Liver HDL receptor mediated endocytosis by liver apoproteins HDL HDL HDL some cholesterol ester transferred to circulating VLDL “used” cholesterol transferred to HDL and converted to cholesterol ester VLDL Cholesterol can be converted to bile salts for excretion or repackaged in VLDL for redistribution Peripheral tissues LDLreceptor mediated endocytosis LDL LDL
High density lipoprotiens HDL • HDL carries “used” cholesterol (as CE) back to the liver. Also donate some CE to circulating VLDL for redistribution to tissues. • HDL taken up by liver and degraded. The cholesterol is excreted as bile salts or repackaged in VLDL for distribution to tissues. • Cholesterol synthesis in the liver is regulated by the cholesterol arriving through HDL (and dietary cholesterol returned by chylomicrons remnants). • Cholesterol (CE) in HDL is referred to as “good cholesterol”
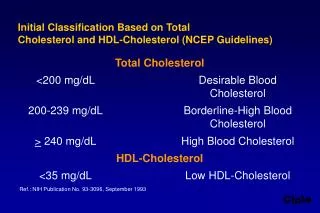
HDL functioning • HDL may transfer some cholesterol esters to other lipoproteins. • Some remain associated with HDL, which may be taken up by liver & degraded. • HDL thus transports cholesterol from tissues & other lipoproteins to the liver, which can excrete excess cholesterol as bile acids. • High blood levels of HDL (the "good" cholesterol) correlate with low incidence of atherosclerosis HDL > 40 mg/dl (NCEP ATP III) “Independent Predictor of CAD”
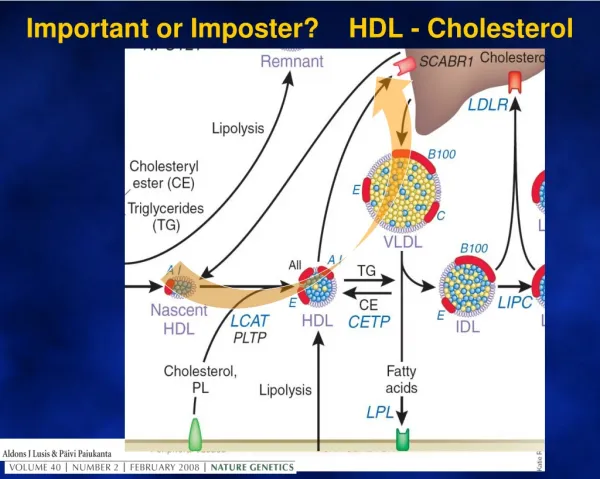
Interrelationship between lipoproteins VLDL CE CETP FFA LPL TG IDL Liver (LDL receptor) TG CETP CE HDL LPL TG FFA CETP Liver (LDL receptor) CE LDL
Reverse Cholesterol Transport: Indirect Extra hepatic tissues Liver Cholesterol is reused or excreted in bile Cholesterol esters hydrolysis Direct Free cholesterol ABCA1 Pre-b-HDL LCAT Cholesterol to VLDL, IDL,LDL CETP HDL A A
Postprandial Changes in Plasma Lipid Metabolism Fat storage via LPL Transfer of cholesterol from cells into plasma reverse transport of cholesterol from peripheral tissue to liver Exchange of cholesterol for VLDL TG in HDL (CETP) LCAT activity = esterification of free cholesterol (HDL) These postprandial changes are beneficial in maintaining whole body homeostasis of glycerides and cholesterol
LCAT deficiency? • CETP deficiency? • Apo AI deficiency?
LDL Liver Dietary fat Bile salts Endogenous cholesterol extra hepatic tissue Exogenous cholesterol small intestine chylomicrons chylomicrons reminants HDL VLDL IDL capillaries Lipoprotein Lipase Lipoprotein Lipase Adipose, muscle FFA FFA
ATHEROSCLEROSIS Normal Atherosclerosis Proliferation of intimal connective tissue Lipid accumulation Tissue breakdown Intima Medis Adventitis Factors such as high plasma cholesterol, smoking, hypertension, diabetes and family history are all associated with atherosclerosis.
Cholesterol ester Monocycle Foam cells LDL Endothelial injury Platelets Role of LDL in atherosclerosis- oxidation
OX-LDL N-LDL B B
LUMEN Endothelium LDL, VLDL Free radicals Free radicals Modified protein & lipid = immunogenicity INTIMA ? Initial Lipoprotein Oxidation Oxidized LDL IEL MEDIA Oxidized LDL Concentration Residence time in arterial wall Opportunity to be oxidized, taken up by macrophage, glycated and be trapped
B B B CE CE CE CE CE CE CE CE CE B B B B B B Tg Tg Tg CE CE CE CE CE CE CE CE CE CE CE CE CE CE CE CE CE CE Tg Tg Tg Tg Tg Tg LDL C 3.5 3.5 Apo B 75 150
LDL apoB Percent 40 30 20 10 0 40 60 80 100 120 140 160 180 200 220 240 260 280 mg/dl LDL cholesterol 25 20 15 10 5 0 mmol/l 1.5 2.0 2.5 3.0 3.5 4.0 4.5 5.0 5.5 6.0 6.5 7.0 7.5 CHD patients Controls small dense LDL is more toxic ( oxidation etc.) but has less cholesterol per particle, measuring LDL cholesterol doesn’t give complete picture. Measuring apoB provides a better index of particle number, and an additional discriminator.
Rupture 7 Endothelium Fatty streak Monocyte LDL Adhesion 1 2 X-LAM LDL M-CSF IL-1 6 Lipid Oxidation MCP-1 MCP-1 Entry 3 5 MM-LDL Oxidation M-CSF Differentiation Smooth muscle cell proliferation Modified LDL uptake Ox-LDL ROS 4 Smooth Muscle cells Macrophage Macrophage induced inflammation
Lumen Intima Fatty lesion (Endothelial damage) Risk factors Regression fibro lipid plaque formation • Fibrous cap • Ground substance • Collagen fibers • Reticulum fibrils Progressive Reduction in blood flow Thrombosis Ulceration 1 2 3 R Smooth Muscle cells Foam cells Calcification 100% Lumen Diameter Intercellular lipid Fatty streak Lipid core Fibrous plaque Haemorrhage Complicated lesion Development of Atherosclerosis
High LDL Levels Receptor Mediated Pathway Non-Specific Anti-oxidant therapy not effective
Relationship between HDL/LDL and heart disease Monocyte (white blood cell) Cholesterol to liver LDL vascular endothelium (+) differentiate Oxidized LDL Arterial Intima Macrophage Role played by Apo A1 LDL (+) (-) HDL Foam cells (fatty streak)
HDL Function • Removal of CE from LDL • Reverse Cholesterol transport • Apo A-1 prevent seeding of LDL • Apo A-1 prevent oxidized LDL formation
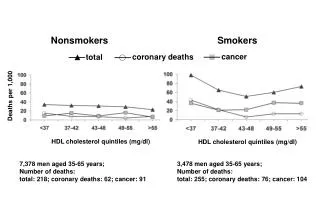
HDL NO More a Good Cholesterol Recent theories • Framingham study of the incidence of coronary heart disease (CHD) & HDL:44% of the events occurred in men with HDL-cholesterol levels of 40 mg/dl and 43% of the events occurred in women with HDL-cholesterol levels of 50 mg/dl • A significant number of CHD events occur in patients with normal LDL-cholesterol levels and normal HDL-cholesterol levels. Search for markers with better predictive value
HDL NO More Good Cholesterol • Increase CHD on high HDL • Good HDL becomes bad (Navab M, 2002) • Conversion of anti-inflammatory HDL into pro-inflammatory HDL Increase risk of atherosclerosis • Dysfunctional HDL has been detected by special test of cell-free assay (Navab M, 2002) • Non-functioning Apo A1 “What makes HDL dysfunctional”?
HDL NO More Good Cholesterol Recent hypotheses • Products of an inflammatory enzyme, myeloperoxidase target main Apo A1 Converting HDL into pro-inflammatory non-functional. • Apo A1 macrophages retain increase cholesterol & cholesterol reverse transport reduced. Myeperoxidase modify tyrosine AA (Fogelman AM 2003) • Dysfunctional HDL has increases hydroperoxidase This makes it pro- inflammatory (Van Lenten et al J. Clin. Invest. 96: 2758–2767 )
HDL NO More Good Cholesterol Role of myeloperoxidase: • Modify tyrosine AA in Apo A-1 100 X more than same AA in other protein • Study: In patients with CHD there is substantial amount of tyrosine AA in Apo A1 modified by myeloperoxidase than in controls(Zheng et al 2004) Why this occur???
Study Rationale Un answered Questions • Which patients are susceptible to develop dysfunctional HDL • What makes myeloperoxidase to cause change in Apo A1 • What is the role of hydroperoxidase in causing dysfunctional HDL
Study Rationale Un answered Questions • Which patients are susceptible to develop dysfunctional HDL • What makes myeloperoxidase to cause change in Apo A1 • What is the role of hydroperoxidase in causing dysfunctional HDL
Study Proposal Objectives are to: • Measure the level of functional & dysfunctional HDL in CHD cases and controls • Assess the risk factors association with dysfunctional HDL in both cases and controls • Measure the levels of myeloperoxidase, hydroperoxidase and Apo A-1 protein in both cases and controls • Study the candidate genes for myeloperoxidase, hydroperoxidase and Apo A-1in cases and controls
Study Proposal Study Design: Case-control Study population: • South Asian Immigrant population residing in San Diego, California (total population- 1500 families) • Number of Groups 1. Hindus: from India, Nepal & SriLanka Ethnic groups: Gujarati, Marathi, Hindi 2. Muslims: from Pakistan, India & Bangladesh
Study Proposal Cases: with known CAD Controls: without CAD Risk factors under study • Traditional risk factors • Emerging risk factors • Myeloperoxidase levels • Hydroperoxidase levels • Apo A-1 levels
Study Proposal Sample size: Biostatistician Data analysis: Multiple logistic regression