Download
1 / 19
210 likes | 817 Views
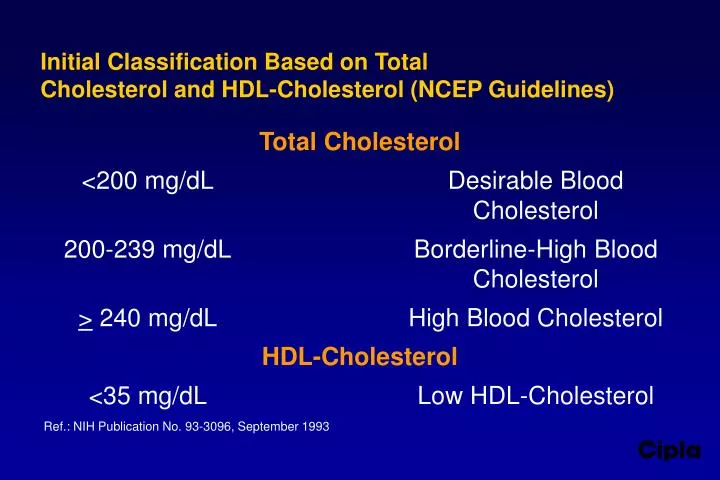
Initial Classification Based on Total Cholesterol and HDL-Cholesterol (NCEP Guidelines). Total Cholesterol <200 mg/dL Desirable Blood Cholesterol 200-239 mg/dL Borderline-High Blood Cholesterol > 240 mg/dL High Blood Cholesterol HDL-Cholesterol <35 mg/dL Low HDL-Cholesterol

E N D
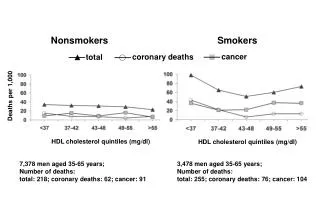
Initial Classification Based on TotalCholesterol and HDL-Cholesterol (NCEP Guidelines) Total Cholesterol <200 mg/dL Desirable Blood Cholesterol 200-239 mg/dL Borderline-High Blood Cholesterol > 240 mg/dL High Blood Cholesterol HDL-Cholesterol <35 mg/dL Low HDL-Cholesterol Ref.: NIH Publication No. 93-3096, September 1993
Treatment Decisions Based on LDL-Cholesterol (NCEP Guidelines) Dietary Therapy Initiation level LDL Goal Without CHD & with fewer than 2 risk factors >160 mg/dL <160 mg/dL Without CHD & with 2 or more risk factors >130 mg/dL <130 mg/dL With CHD >100 mg/dL <100 mg/dL Drug Treatment Consideration LDL Goal Level Without CHD & with fewer than 2 risk factors >190 mg/dL* <160 mg/dL Without CHD & with 2 or more risk factors >160 mg/dL <130 mg/dL With CHD >130 mg/dL** <100 mg/dL *In men under 35 years of age and premenopausal women with LDL-cholesterol levels 190-219 mg/dL, drug therapy should be delayed except in high-risk patients such as those with diabetes. **In CHD patients with LDL-cholesterol levels 100-219 mg/dL, the physician should exercise clinical judgement in deciding whether to initiate drug treatment. Ref.: NIH Publication No. 93-3096, September 1993
CHD Risk Factors • Positive • Age s Smoking • Male > 45 years s Hypertension • Female > 55 years or s HDL-cholesterolpremature menopause without < 35 mg/dLestrogen replacement therapy s Diabetes • Family history of premature CHD • Negative • HDL-cholesterol > 60 mg/dL
Effect of Statins on CardiovascularEvent Reduction and LDL-Cholesterol Levels Clinical Active Dosage, Study Baseline % On-treatment CHD Trial Treatment mg/d Sample LDL-C Reduction LDL-C, Red- size Levels, of LDL-C mmol/L uction mmol/L % WOSCOPS Pravastatin 40 6595 4.97 26 3.87 31 PLAC II Pravastatin 20-40 151 4.29 27 3.10 60 REGRESS Pravastatin 40 885 4.32 28 3.03 42 CARE Pravastatin 40 4159 3.59 28 2.59 24 CCAIT Lovastatin 40-80 331 4.47 29 3.26 25 MAAS Simvastatin 20 381 4.40 31 3.00 24 4S Simvastatin 20-40 4444 4.87 34 3.15 34 MARS Lovastatin 80 270 3.90 38 2.40 24 JAMA 1998; 279: 1643-1650.
Vascular mechanisms by which cholesterol lowering may reduce coronary events Potential Beneficial Effects Of Lipid Lowering Cells Present in Atheroma Endothelial Dependent Vasodilation - ¯ Superoxide (O ) Production 2 ¯ Leukocyte Adhesion Molecule Expression Endothelial Cell ¯ Secretion of Matrix-Degrading Proteases ¯ Release of Inflammatory Cytokines Macrophage ¯ Procoagulant Tissue Factor Expression Foam-Cell ¯ Growth Factor Production Smooth ¯ Macrophage Stimulator Muscle Production (M-CSF & MCP-1) Cell ¯ Modified Lipoprotein Antigen Stimulation ¯ Production of Gamma Interferon (a macrophage stimulator and matrix T-Lymphocyte synthesis inhibitor)
Simvastatin - Pharmacodynamics • Orally administered prodrug, hydrolysed to b-hydroxyacid simvastatin, the active metabolite • Potent inhibitor of cholesterol biosynthesis • Upregulates LDL receptors • Reduces total cholesterol, LDL cholesterol, triglycerides & increases HDL cholesterol • Decreases apolipoprotein B and increases apolipoproteins AI and AII • Inhibits platelet activation, decreases factor VIIc activity, produces modest reduction or no change in fibrinogen levels • Unlikely to alter adrenal function • Does not increase cataract formation SIMCARD
4S Trial: Summary Parameter % Reduction Total cholesterol 25% LDL cholesterol 35% Triglycerides 10% Total mortality 30% Coronary mortality 42% Non-fatal acute MI 37% Cerebrovascular events 30% Revascularisation procedures 37% No. of hospital admissions 26% Average length of stay 10% Total days spent in hospital 34% SIMCARD Ref.: Lancet 1994; 344:1383-1389.
LIFE SAVING BENEFITS OF SIMVASTATIN MAINTAINED FOR UP TO EIGHT YEARS • 30% reduction in mortality observed during 5-year study maintained during the extended two-year follow-up of 4S trial % Mortality - 71st Scientific Sessions of American Heart Association, Nov 1998
Simvastatin approved by US FDA inpatients with elevated triglyceride levels Results of analysis of 5 studies (n=359) Baseline triglyceride Percentage reduction levels with simvastatin TG > 200 mg/dL 31% TG 150-200 mg/dL 21% TG < 150 mg/dL 11% SCRIP 1997; No. 2284:19 SIMCARD
Simvastatin approved for use in patients with isolated hypertriglyceridemia (Frederickson type IV) and in patients with type III hyperlipoproteinemiaInpharma 1999; 1218: 22
Main angiographic findings of the Multicentre Anti-Atheroma Study (MAAS)after 4 years of treatment with simvastatin 20 mg/day Angiographic parameter Angiographic classification (per patient) (per patient) [mean change [no. (%) of patients] from baseline] simvastatin placebo simvastatin placebo Diffuse disease Mean lumen –0.02 –0.08* diameter (mm) Focal disease Minimum lumen –0.04 –0.13** diameter (mm) Diameter stenosis (%) 1.0 3.6** Progressor 41 (23.0) 54 (32.3)*a Regressor 33 (18.6) 20 (12.0)*a a Statistically significant difference between treatment groups only for combined treatment effect.Statistically significant difference between treatment groups: *p < 0.05, **p < 0.01 Ref.: Lancet 1994; 344: 633-638. SIMCARD
SIMVASTATIN/ENALAPRIL CORONARY ATHEROSCLEROSIS TRIAL (SCAT) • 460 patients with normal cholesterol levels (160 mg/dl - 240 mg/dl) and established CAD • Simvastatin significantly reduced LDL cholesterol, total cholesterol and triglycerides and increased HDL cholesterol • Simvastatin reduced need for revascularisation procedures by 53.6%; need for angioplasty was reduced by 61.9% • Addition of enalapril to the regimen had a neutral impact on the progression of CAD Simvastatin slows CAD progression in patients of normal cholesterol - 48th Annual Scientific Sessions of American College of Cardiology, March 1999
EFFECT OF SIMVASTATIN ON HEART FAILURE (SUBSET ANALYSIS OF 4S TRIAL) Patients withheart failure (%) - Journal of Failure 1997; 3: 249-254
SIMVASTATIN APPROVED BY US FDA FOR RAISING HDL LEVELS • New approval based on four studies • In one study (n=130), simvastatin lowered LDL cholesterol by 29-36%, triglycerides by 28-33% and raised HDL levels by 13-16% • HDL is anti-atherogenic; high levels of HDL reduce CHD risk • HDL-C > 60mg/dl is a negative risk factor for CHD and HDL-C < 35 mg/dl is a positive risk factor for CHD (NCEP guidelines) - SCRIP 1999; 2463: 19
Safety of simvastatin Common adverse effects include • increase in liver enzymes • myopathy (increase in creatine kinase) • GI problems • CNS disturbances Discontinuation rates : 0.3 to 0.7% SIMCARD Ref.: Annals of Pharmacotherapy 1995; 29:743-759.
Simvastatin Vs. Lovastatin (Twice as potent) Reference No. of Dosage Mean percentage change in serum lipid/ evaluable regimen lipoprotein levels versus baselinea patients (mg/day) Total-C LDL-C HDL-C TG LDL-C/ HDL-C Farmer 134 S10 -19.6 -27.5 +4.6 -3.9 -29.5et al 135 S20 -25.4*b -34.7*b +4.6 -10.3 -37.1*b(24-week 137 L20 -18.6 -25.4 +4.2 -10.5 -27.4study) 134 L40 -22.6 -31.2 +7.4 -10.3 -34.9 Frohlich 149 S10-40 -26 to -34 to +8 -16 toet al -30 -37 -17(18-week 149 L20-80 -26 to -34 to +4 to -11 tostudy) -31 -38 +10 -22 S=Simvastatin; L=Lovastatin; a All changes in total-C & LDL-C were statistically significant compared with baseline, b Statistically significant difference between treatment groups refers to S 20 versus L20. *indicates p < 0.01. SIMCARD - Drugs 1995; 50(2): 334-363. - Can. J. Cardiol. 1993; 9:405-412.
Simvastatin Vs. Lovastatin (Greater percentage of responders) % of patients with LDL Cholesterol< 130 mg/dL at 18 weeks SIMCARD Ref.: Annals of Pharmacotherapy 1995; 29: 743-759.
Simvastatin vs. Lovastatin(Contd.) Adverse Event % incidence of adverse events Simvastatin Lovastatin 20 mg twice daily 20 mg twice daily (n=84) (n=42) Headaches 3.6% 7.1% Abdominal discomfort 2.4% 4.8% Sleep disorders 3.6% 7.1% Muscle pain 2.4% 4.8% in creatine kinase 4.8% 11.9% in liver enzymes 4.8% 11.9% Discontinuation rates with simvastatin have been reported to range between 0.3 and 0.7% as compared to 2.8 to 4% with lovastatin. SIMCARD
Simvastatin: Dosage and Administration • The recommended starting dose is 5-10 mg once daily in the evening. Doses should be individualised according to baseline LDL cholesterol levels and the LDL goal recommended by the NCEP. Patients requiring reductions in LDL-C of 20% or more to achieve their goal should be started on 10 mg/day. A starting dose of 5 mg should be considered for patients requiring smaller reduction in LDL-C, for the elderly and in patients with severe renal insufficiency • The recommended dosing range is 5-80 mg/day; the maximum recommended dose is 80 mg/day • Adjustments of dosage should be made at intervals of 4 weeks or more