Download
1 / 40
890 likes | 1.27k Views
The Basic Science of Heart Failure: Dual-Action Molecules in Perspective. Adverse Neurohormonal Activation in HF Has Formed the Basis for Evidence-Based Pharmacologic Therapy. Renin-Angiotensin-Aldosterone System. RAAS Inhibition in CHF.

E N D
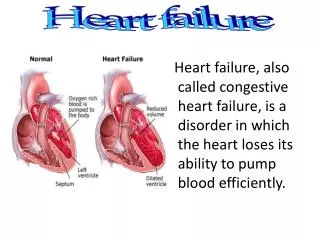
The Basic Science of Heart Failure: Dual-Action Molecules in Perspective
Adverse Neurohormonal Activation in HF Has Formed the Basis for Evidence-Based Pharmacologic Therapy
Effect of ACE Inhibition in Patients With CHF: CONSENSUS Trial
ATMOSPHERE: Would Dual Blockade of the RAS With Evidence-Based Background Therapy Be Superior to Single-Agent RAS Inhibition?
ATMOSPHERE: Direct Renin Inhibition and ACE Inhibition Similar: DUAL Inhibition NO BETTER and Produced More Side Effects
NP System: Endogenous Compensatory Mechanisms in HF Counteract Some Deleterious Effects of RAAS Activation
Sacubitril/Valsartan: ARNI—Simultaneously Inhibits RAS and Augments Vasoactive Peptides
PARADIGM-HF Primary Results: Significant Reduction in Primary Endpoints, CV Death, andAll-Cause Mortality
PARADIGM-HF: Sacubitril/Valsartan (LCZ696) vs Enalapril on Primary Endpoint and on CV Death, by Subgroups
PARADIGM-HF: Sacubitril/Valsartan Effective Across a Spectrum of Risk: The MAGGIC Risk Score
Influence of Sacubitril/Valsartan on 30-Day Readmission After HF Hospitalization
Estimated Long-term Benefit of 1.5-2 Years Using Actuarial Methods: Based on PARADIGM-HF
Potential Mortality Reduction With Optimal Implementation of ARNI Therapy in HF
Sacubitril/Valsartan Was Effective Across the Spectrum of EF: PARADIGM-HF Enrolled >2000 Patients With EF Between 35% and 40%
PARADIGM-HF: Comparison of Sacubitril/Valsartan vs Enalapril in Dose-Reduced Patients
No Heterogeneity in Treatment Effect by NT-proBNP at Baseline
PARADIGM-HF: Influence of Sacubitril/Valsartan on NT-proBNP Reduction and Influence on Outcomes
PARAMOUNT: Designed in Parallel With PARADIGM-HF to Provide Pilot Data for Sacubitril/Valsartan in HFpEF
PARAMOUNT: Significant Reduction in NT-proBNP With Sacubitril/Valsartan at 12 Weeks
PARAMOUNT: Improvement in Left Atrial Size and NYHA Class With Sacubitril/Valsartan at 36 Weeks