Download
1 / 1
10 likes | 77 Views
Risk of clinical dementia: cortical, hippocampal and entorhinal pathologies. Less common and “disregarded” pathologies in late onset dementia: what are we missing? Hannah A .D. Keage 1,2 , Paul G. Ince 3 , Fiona E. Matthews 4 , Stephen B Wharton 3 , Ian McKeith 5 and Carol Brayne 2

E N D
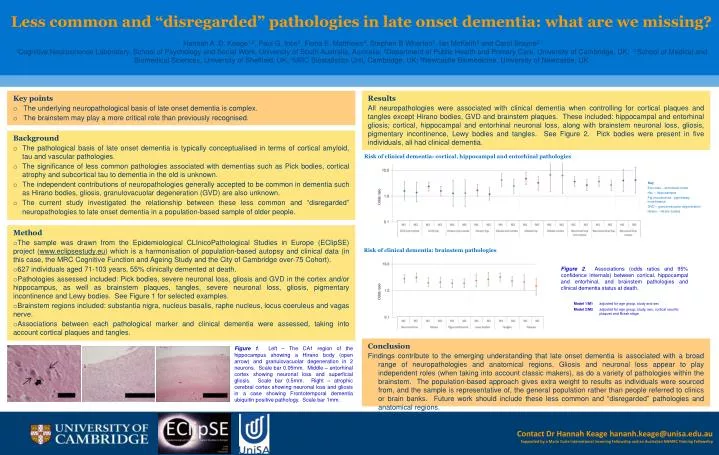
Risk of clinical dementia: cortical, hippocampal and entorhinal pathologies Less common and “disregarded” pathologies in late onset dementia: what are we missing? Hannah A .D. Keage1,2, Paul G. Ince3, Fiona E. Matthews4, Stephen B Wharton3, Ian McKeith5 and Carol Brayne2 1Cognitive Neuroscience Laboratory, School of Psychology and Social Work, University of South Australia, Australia; 2Department of Public Health and Primary Care, University of Cambridge, UK; 3School of Medical and Biomedical Sciences, University of Sheffield, UK;4MRC Biostatistics Unit, Cambridge, UK; 5Newcastle Biomedicine, University of Newcastle, UK Odds ratio Risk of clinical dementia: brainstem pathologies Odds ratio Results All neuropathologies were associated with clinical dementia when controlling for cortical plaques and tangles except Hirano bodies, GVD and brainstem plaques. These included: hippocampal and entorhinal gliosis; cortical, hippocampal and entorhinal neuronal loss, along with brainstem neuronal loss, gliosis, pigmentary incontinence, Lewy bodies and tangles. See Figure 2. Pick bodies were present in five individuals, all had clinical dementia. • Key points • The underlying neuropathological basis of late onset dementia is complex. • The brainstem may play a more critical role than previously recognised. • Background • The pathological basis of late onset dementia is typically conceptualised in terms of cortical amyloid, tau and vascular pathologies. • The significance of less common pathologies associated with dementias such as Pick bodies, cortical atrophy and subcortical tau to dementia in the old is unknown. • The independent contributions of neuropathologies generally accepted to be common in dementia such as Hirano bodies, gliosis, granulovacuolar degeneration (GVD) are also unknown. • The current study investigated the relationship between these less common and “disregarded” neuropathologies to late onset dementia in a population-based sample of older people. Key Ent.cotex – entorhinal cortex Hip. – hippocampus Pig.incontinence - pigmentary incontinence GVD – granulovacuolar degeneration Hirano – Hirano bodies • Method • The sample was drawn from the Epidemiological CLInicoPathological Studies in Europe (EClipSE) project (www.eclipsestudy.eu) which is a harmonisation of population-based autopsy and clinical data (in this case, the MRC Cognitive Function and Ageing Study and the City of Cambridge over-75 Cohort). • 627 individuals aged 71-103 years, 55% clinically demented at death. • Pathologies assessed included: Pick bodies, severe neuronal loss, gliosis and GVD in the cortex and/or hippocampus, as well as brainstem plaques, tangles, severe neuronal loss, gliosis, pigmentary incontinence and Lewy bodies. See Figure 1 for selected examples. • Brainstem regions included: substantia nigra, nucleus basalis, raphe nucleus, locus coeruleus and vagas nerve. • Associations between each pathological marker and clinical dementia were assessed, taking into account cortical plaques and tangles. Figure 2. Associations (odds ratios and 95% confidence internals) between cortical, hippocampal and entorhinal, and brainstem pathologies and clinical dementia status at death. Model 1/M1 adjusted for age group, study and sex Model 2/M2 adjusted for age group, study, sex, cortical neuritic plaques and Braak stage Conclusion Findings contribute to the emerging understanding that late onset dementia is associated with a broad range of neuropathologies and anatomical regions. Gliosis and neuronal loss appear to play independent roles (when taking into account classic makers), as do a variety of pathologies within the brainstem. The population-based approach gives extra weight to results as individuals were sourced from, and the sample is representative of, the general population rather than people referred to clinics or brain banks. Future work should include these less common and “disregarded” pathologies and anatomical regions. Figure 1. Left – The CA1 region of the hippocampus showing a Hirano body (open arrow) and granulovacuolar degeneration in 2 neurons. Scale bar 0.05mm. Middle – entorhinal cortex showing neuronal loss and superficial gliosis. Scale bar 0.5mm. Right – atrophic cerebral cortex showing neuronal loss and gliosis in a case showing Frontotemporal dementia ubiquitin positive pathology. Scale bar 1mm. Contact Dr Hannah Keage hananh.keage@unisa.edu.au Supported by a Marie Curie International Incoming Fellowship and an Australian NHMRC Training Fellowship






















