Download
1 / 1
10 likes | 161 Views
Revision Total Knee Arthroplasty Using Femoral Head Structural Allograft Corey J. Richards, MD, MASc, FRCSC Luke Pugh, MD Donald S. Garbuz, MD, MHSc, FRCSC Nelson V. Greidanus, MD, MPH, FRCSC Bassam A. Masri, MD, FRCSC. Purpose. Introduction.

E N D
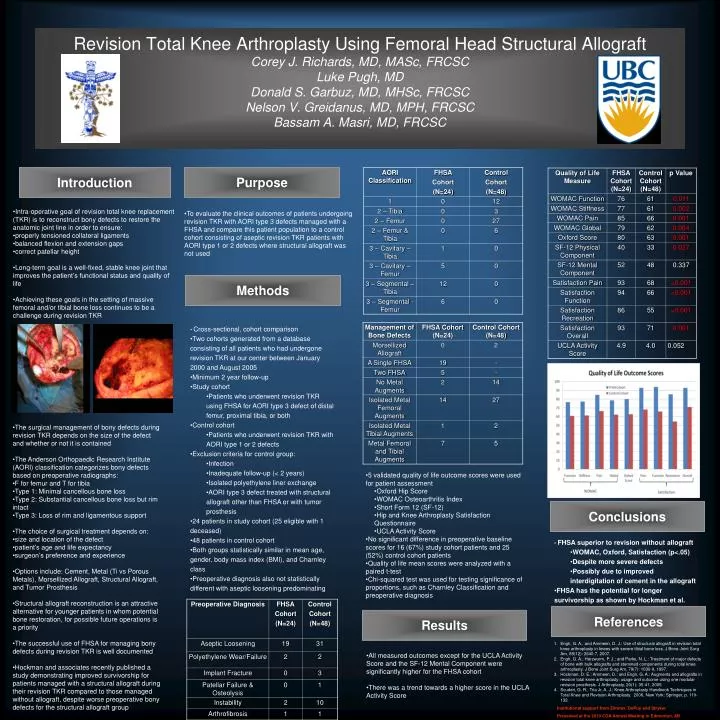
Revision Total Knee Arthroplasty Using Femoral Head Structural AllograftCorey J. Richards, MD, MASc, FRCSCLuke Pugh, MDDonald S. Garbuz, MD, MHSc, FRCSCNelson V. Greidanus, MD, MPH, FRCSCBassam A. Masri, MD, FRCSC Purpose Introduction • To evaluate the clinical outcomes of patients undergoing revision TKR with AORI type 3 defects managed with a FHSA and compare this patient population to a control cohort consisting of aseptic revision TKR patients with AORI type 1 or 2 defects where structural allograft was not used • Intra-operative goal of revision total knee replacement (TKR) is to reconstruct bony defects to restore the anatomic joint line in order to ensure: • properly tensioned collateral ligaments • balanced flexion and extension gaps • correct patellar height • Long-term goal is a well-fixed, stable knee joint that improves the patient’s functional status and quality of life • Achieving these goals in the setting of massive femoral and/or tibial bone loss continues to be a challenge during revision TKR Methods • Cross-sectional, cohort comparison • Two cohorts generated from a database consisting of all patients who had undergone revision TKR at our center between January 2000 and August 2005 • Minimum 2 year follow-up • Study cohort • Patients who underwent revision TKR using FHSA for AORI type 3 defect of distal femur, proximal tibia, or both • Control cohort • Patients who underwent revision TKR with AORI type 1 or 2 defects • Exclusion criteria for control group: • Infection • Inadequate follow-up (< 2 years) • Isolated polyethylene liner exchange • AORI type 3 defect treated with structural allograft other than FHSA or with tumor prosthesis • 24 patients in study cohort (25 eligible with 1 deceased) • 48 patients in control cohort • Both groups statistically similar in mean age, gender, body mass index (BMI), and Charnley class • Preoperative diagnosis also not statistically different with aseptic loosening predominating • The surgical management of bony defects during revision TKR depends on the size of the defect and whether or not it is contained • The Anderson Orthopaedic Research Institute (AORI) classification categorizes bony defects based on preoperative radiographs: • F for femur and T for tibia • Type 1: Minimal cancellous bone loss • Type 2: Substantial cancellous bone loss but rim intact • Type 3: Loss of rim and ligamentous support • The choice of surgical treatment depends on: • size and location of the defect • patient’s age and life expectancy • surgeon’s preference and experience • Options include: Cement, Metal (Ti vs Porous Metals), Morsellized Allograft, Structural Allograft, and Tumor Prosthesis • Structural allograft reconstruction is an attractive alternative for younger patients in whom potential bone restoration, for possible future operations is a priority • The successful use of FHSA for managing bony defects during revision TKR is well documented • Hockman and associates recently published a study demonstrating improved survivorship for patients managed with a structural allograft during their revision TKR compared to those managed without allograft, despite worse preoperative bony defects for the structural allograft group • 5 validated quality of life outcome scores were used for patient assessment • Oxford Hip Score • WOMAC Osteoarthritis Index • Short Form 12 (SF-12) • Hip and Knee Arthroplasty Satisfaction Questionnaire • UCLA Activity Score • No significant difference in preoperative baseline scores for 16 (67%) study cohort patients and 25 (52%) control cohort patients • Quality of life mean scores were analyzed with a paired t-test • Chi-squared test was used for testing significance of proportions, such as Charnley Classification and preoperative diagnosis Conclusions • FHSA superior to revision without allograft • WOMAC, Oxford, Satisfaction (p<.05) • Despite more severe defects • Possibly due to improved interdigitation of cement in the allograft • FHSA has the potential for longer survivorship as shown by Hockman et al. References Results • Engh, G. A., and Ammeen, D. J.: Use of structural allograft in revision total knee arthroplasty in knees with severe tibial bone loss. J Bone Joint Surg Am, 89(12): 2640-7, 2007. • Engh, G. A.; Herzwurm, P. J.; and Parks, N. L.: Treatment of major defects of bone with bulk allografts and stemmed components during total knee arthroplasty. J Bone Joint Surg Am, 79(7): 1030-9, 1997. • Hockman, D. E.; Ammeen, D.; and Engh, G. A.: Augments and allografts in revision total knee arthroplasty: usage and outcome using one modular revision prosthesis. J Arthroplasty, 20(1): 35-41, 2005. • Scuderi, G. R.; Tria Jr, A. J.: Knee Arthroplasty Handbook Techniques in Total Knee and Revision Arthroplasty. 2006, New York: Springer, p. 119-132. • All measured outcomes except for the UCLA Activity Score and the SF-12 Mental Component were significantly higher for the FHSA cohort • There was a trend towards a higher score in the UCLA Activity Score Institutional support from Zimmer, DePuy and Stryker Presented at the 2010 COA Annual Meeting in Edmonton, AB