Download
1 / 131
1.37k likes | 1.82k Views
Steven L. Frick, MD Carolinas Medical Center Charlotte, NC. Pediatric Hip. Pediatric Hip Problems. Common, age related differences in presentation Traction rarely used now as treatment If used, often in-line skin traction (Buck’s) for comfort temporarily

E N D
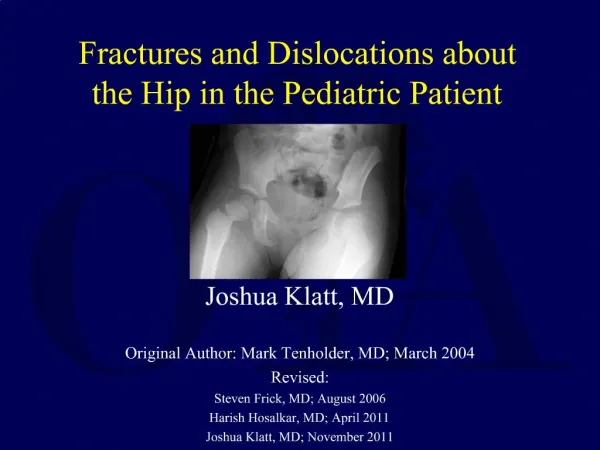
Steven L. Frick, MD Carolinas Medical Center Charlotte, NC Pediatric Hip
Pediatric Hip Problems • Common, age related differences in presentation • Traction rarely used now as treatment • If used, often in-line skin traction (Buck’s) for comfort temporarily • Remember to limit weight, watch skin • DDH, LCP, SCFE, trauma
Developmental Hip DysplasiaDDH- definition • Developmental instead of congenital- more reflective of etiology • Any hip which can be provoked to subluxate (partial contact between femoral head and acetabulum) or dislocate (no contact between femoral head and acetabulum), or any subluxated or dislocated hip that can be reduced
DDH Incidence • Depends on criteria • 2-9/1000 births • 70% female • Left > Right, 20% bilateral • some populations at higher risk
Risk Factors • 1st born • Female • Breech • + family history • Torticollis, MTA – some debate • Some populations- swaddling
Treatment Goals • Obtain and maintain reduction to provide optimal environment for hip development • Potential for remodeling/development present for many years • Intervene to alter otherwise unfavorable natural history • AVOID ischemic necrosis
Treatment: Newborn - 6 mo. CR => Pavlik harness • Arnold Pavlik, MD 1945 • “functional” treatment • 531/632 dislocated hips reduced with no AVN
Pavlik Harness Mubarak et al. – JBJS 1981- Pitfalls
Success-Pavlik Harness • Dislocated- 85% • Dislocatable- 95-100% • Residual Dysplasia- may have acetabular dysplasia in up to 15% after successful reduction/stabilization
“Failed Pavlik” Hip • Arthrogram • closed vs. open reduction • spica cast 6-12 weeks • Can try rigid abduction bracing- about 50% of Pavlik failures will dock and stabilize
Plastizote abduction brace for failed Pavlik harness reduction • >50% success at reduction • Boston Children’s series 13/15 success
Ultrasound • Static angles (Graf) • % fem head coverage (Morin – 58% normal) • Dynamic stability (Harcke)
Ultrasound - DynamicHarcke Evaluate stability, real time, no radiation, document success/failure of reduction, easy to perform in harness
Ultrasound Disadvantages • Only < 9mos (ossific nucleus) • Expense • Technique/expertise dependent • not good at quantifying dysplasia • May lead to overtreatment (stable hips dysplastic by US become normal)
Newborn male B dislocated hips • Pavlik for 4 weeks • Ultrasound to document reduction
Keep Hip in Socket while... Avoiding AVN is goal
To assess closed reduction after spica cast : Check CT scan or MRI scan
Open Reduction • For failure to achieve acceptable closed reduction, late presentation (>18 mos) • Anterior (capsulorrhaphy) or anteromedial (remove obstacles, no capsulorrhaphy) • Higher % ON (mild) with anteromedial approach
Follow until skeletal maturity • Make sure acetabulum develops properly • Goal = normal motion and normal radiograph at maturity • radiographic assessment 6-12 mo intervals, then 2-3 year intervals • acetabular index, lateralization ratio, teardrop, subluxation, femoral head ossification
42 months 21 months 38 years 24 years Courtesy of S. Weinstein, MD Univ. of Iowa
Persistent Acetabular Dysplasia • Scoles – normal values for AI- 20 deg by 2 yrs • Lindseth/Ponseti/Wenger – acetabular development may proceed up to age 8 after CR • Lalonde/Frick/Wenger – residual hip dysplasia treated < age 8 more normal radiographic anatomy • AI>35 2 yrs post CR- 80% Severin III or IV
Subluxation • Those with subluxation more symptomatic • Usually symptomatic by mid 30’s for women
Salter Pelvic Osteo-tomy • Redirects acetabulum to give more coverage to femoral head
Exam - Older Infant > 3 Months • Limited abduction • Asymmetric thigh folds • Galeazzi or Allis sign- short femoral segment with hip and knee flexed
Limited Abduction Galeazzi sign
4 yr old missed bilat DDH Waddling gait Lumbar lordosis Trendelenberg
DDH Older child • Treatment principles the same • reduce hip without excessive pressure • operative treatment • shorten femur – traction out of favor • femoral and pelvic osteotomies • older, bilateral - ? No treatment • Unilateral – up to age 10, bilateral age 6