Download
1 / 1
10 likes | 103 Views
Treatment-related reduction in HIV sexual risk behavior: A CTN secondary analysis T Killeen 1 , R Carter 1 , M Stitzer 2 , G Woody 3 , M Copersino 4 , J Roll 5 , R Booth 6

E N D
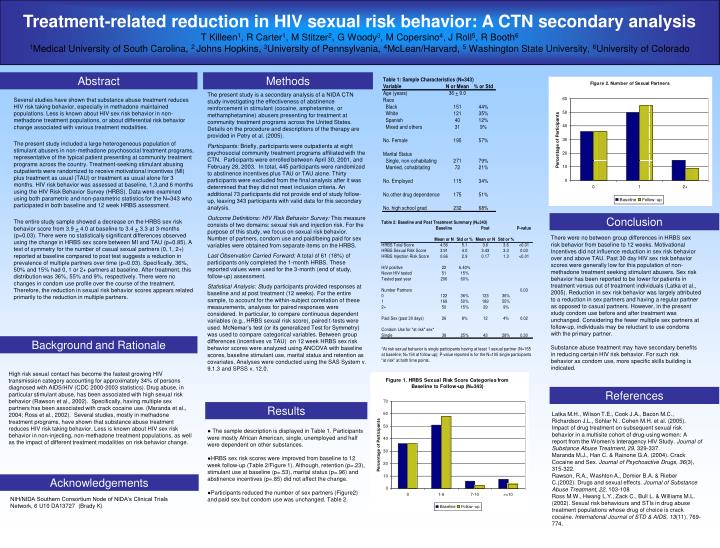
Treatment-related reduction in HIV sexual risk behavior: A CTN secondary analysis T Killeen1, R Carter1, M Stitzer2, G Woody3, M Copersino4, J Roll5, R Booth6 1Medical University of South Carolina, 2 Johns Hopkins, 3University of Pennsylvania, 4McLean/Harvard, 5 Washington State University, 6University of Colorado Abstract Methods The present study is a secondary analysis of a NIDA CTN study investigating the effectiveness of abstinence reinforcement in stimulant (cocaine, amphetamine, or methamphetamine) abusers presenting for treatment at community treatment programs across the United States. Details on the procedure and descriptions of the therapy are provided in Petry et al. (2005). Participants: Briefly, participants were outpatients at eight psychosocial community treatment programs affiliated with the CTN. Participants were enrolled between April 30, 2001, and February 28, 2003. In total, 445 participants were randomized to abstinence incentives plus TAU or TAU alone. Thirty participants were excluded from the final analysis after it was determined that they did not meet inclusion criteria. An additional 73 participants did not provide end of study follow-up, leaving 343 participants with valid data for this secondary analysis. Outcome Definitions: HIV Risk Behavior Survey: This measure consists of two domains: sexual risk and injection risk. For the purpose of this study, we focus on sexual risk behavior. Number of partners, condom use and paid/being paid for sex variables were obtained from separate items on the HRBS. Last Observation Carried Forward: A total of 61 (18%) of participants only completed the 1-month HRBS. These reported values were used for the 3-month (end of study, follow-up) assessment. Statistical Analysis: Study participants provided responses at baseline and at post treatment (12 weeks). For the entire sample, to account for the within-subject correlation of these measurements, analyses for paired responses were considered. In particular, to compare continuous dependent variables (e.g., HRBS sexual risk score), paired t-tests were used. McNemar’s test (or its generalized Test for Symmetry) was used to compare categorical variables. Between group differences (incentives vs TAU) on 12 week HRBS sex risk behavior scores were analyzed using ANCOVA with baseline scores, baseline stimulant use, marital status and retention as covariates. Analyses were conducted using the SAS System v. 9.1.3 and SPSS v. 12.0. Several studies have shown that substance abuse treatment reduces HIV risk taking behavior, especially in methadone maintained populations. Less is known about HIV sex risk behavior in non-methadone treatment populations, or about differential risk behavior change associated with various treatment modalities. The present study included a large heterogeneous population of stimulant abusers in non-methadone psychosocial treatment programs, representative of the typical patient presenting at community treatment programs across the country. Treatment-seeking stimulant abusing outpatients were randomized to receive motivational incentives (MI) plus treatment as usual (TAU) or treatment as usual alone for 3 months. HIV risk behavior was assessed at baseline, 1,3,and 6 months using the HIV Risk Behavior Survey (HRBS). Data were examined using both parametric and non-parametric statistics for the N=343 who participated in both baseline and 12 week HRBS assessment. The entire study sample showed a decrease on the HRBS sex risk behavior score from 3.9 + 4.0 at baseline to 3.4 + 3.3 at 3-months (p=0.03). There were no statistically significant differences observed using the change in HRBS sex score between MI and TAU (p=0.85). A test of symmetry for the number of casual sexual partners (0, 1, 2+) reported at baseline compared to post test suggests a reduction in prevalence of multiple partners over time (p=0.03). Specifically, 36%, 50% and 15% had 0, 1 or 2+ partners at baseline. After treatment, this distribution was 36%, 55% and 9%, respectively. There were no changes in condom use profile over the course of the treatment. Therefore, the reduction in sexual risk behavior scores appears related primarily to the reduction in multiple partners. Conclusion There were no between group differences in HRBS sex risk behavior from baseline to 12 weeks. Motivational Incentives did not influence reduction in sex risk behavior over and above TAU. Past 30 day HIV sex risk behavior scores were generally low for this population of non-methadone treatment seeking stimulant abusers. Sex risk behavior has been reported to be lower for patients in treatment versus out of treatment individuals (Latka et al., 2005). Reduction in sex risk behavior was largely attributed to a reduction in sex partners and having a regular partner as opposed to casual partners. However, in the present study condom use before and after treatment was unchanged. Considering the fewer multiple sex partners at follow-up, individuals may be reluctant to use condoms with the primary partner. Substance abuse treatment may have secondary benefits in reducing certain HIV risk behavior. For such risk behavior as condom use, more specific skills building is indicated. Background and Rationale High risk sexual contact has become the fastest growing HIV transmission category accounting for approximately 34% of persons diagnosed with AIDS/HIV (CDC 2000-2003 statistics). Drug abuse, in particular stimulant abuse, has been associated with high sexual risk behavior (Rawson et al., 2002). Specifically, having multiple sex partners has been associated with crack cocaine use. (Maranda et al., 2004; Ross et al., 2002). Several studies, mostly in methadone treatment programs, have shown that substance abuse treatment reduces HIV risk taking behavior. Less is known about HIV sex risk behavior in non-injecting, non-methadone treatment populations, as well as the impact of different treatment modalities on risk behavior change. References Results Latka M.H., Wilson T.E., Cook J.A., Bacon M.C., Richardson J.L., Sohlar N.. Cohen M.H. et al. (2005). Impact of drug treatment on subsequent sexual risk behavior in a multisite cohort of drug-using women: A report from the Women’s Interagency HIV Study. Journal of Substance Abuse Treatment, 29, 329-337. Maranda M.J., Han C. & Rainone G.A. (2004). Crack Cocaine and Sex. Journal of Psychoactive Drugs, 36(3), 315-322. Rawson, R.A., Washton A., Domier B.A. & Rieber C.(2002). Drugs and sexual effects. Journal of Substance Abuse Treatment, 22, 103-108 Ross M.W., Hwang L.Y., Zack C., Bull L. & Williams M.L. (2002). Sexual risk behaviours and STIs in drug abuse treatment populations whose drug of choice is crack cocaine. International Journal of STD & AIDS, 13(11), 769-774. ● The sample description is displayed in Table 1. Participants were mostly African American, single, unemployed and half were dependent on other substances. ●HRBS sex risk scores were improved from baseline to 12 week follow-up (Table 2/Figure 1). Although, retention (p=.23), stimulant use at baseline (p=.53), marital status (p=.96) and abstinence incentives (p=.85) did not affect the change. ●Participants reduced the number of sex partners (Figure2) and paid sex but condom use was unchanged. Table 2. Acknowledgements NIH/NIDA Southern Consortium Node of NIDA’s Clinical Trials Network, 6 U10 DA13727 (Brady K)