Download
1 / 17

E N D
1. The Management of People at High Risk of CVD Dr Richard Healicon
Mel Varvel
NHS Improvement
2. Introduction The challenge
Meeting the challenge
Click here to look inside
Your opportunity to contribute
3. Rationale for CVD Prevention CVD is a major cause of mortality & morbidity & is a significant drain on health care resources
Underlying atherosclerosis develops insidiously over many years & is usually advanced by the time symptoms occur
Death from CVD often occurs suddenly & before medical care is available so that therapeutic interventions are either inapplicable or palliative
Prevalence of CVD relates strongly to lifestyles & modifiable physiological & biochemical factors
Risk factor modifications have been shown to reduce CVD mortality & morbidity, particularly in high risk subjects
4. Management of high risk people Continued confusion about whether people at high risk are eligible/stay in the programme
People on statins are excluded because they will have already had a risk assessment and should be managed according to NICE guidelines.
People who are found to be at or above 20% risk should exit the programme irrespective of whether they have signs of disease
People at or above 20% risk without disease should be placed on a high risk register and managed accordingly
Work with NHS I to improve use of high risk registers and management of high risk people about to start
5. Policy Context: NHS Health Check
6. Policy Context: NSF for CHD Standard four: General practitioners and primary health care teams should identify all people at significant risk of cardiovascular disease but who have not yet developed symptoms and offer them appropriate advice and treatment to reduce their risks.
Milestone 2:
Every practice should have:
a systematically developed and maintained practice-based register of people with clinical evidence of CHD, occlusive vascular disease AND of people whose risk of CHD events is > 30% over ten years in place and actively used to provide structured care to those at high risk of CHD.
7. Policy Context: NSF for CHD Milestone 3:
Every practice should have:
a protocol describing the systematic assessment, treatment and follow-up of people at high risk of CHD, including those without evidence of existing arterial disease but whose risk of CHD events is > 30% over ten years, agreed locally and being used to provide structured care to people with CHD.
Milestone 4: Every practice should have:
clinical audit data no more than 12 months old available that describes all the items listed in paragraph 13 on page 4 [see CHD NSF Chapter Two].
The NSF goal: Every practice should:
offer advice about each of the specified effective interventions to all of those in whom they are indicated, demonstrated by clinical audit data no more than 12 months old.
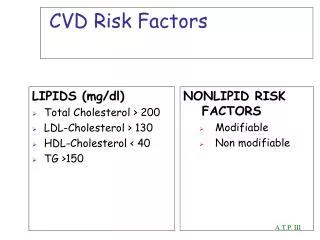
8. Existing Guidelines: JBS2 We recommend that CVD prevention in clinical practice should focus equally on
(i) people with established atherosclerotic CVD,
(ii) people with diabetes, and
(iii) apparently healthy individuals at high risk (CVD risk of > 20% over 10 years) of developing symptomatic atherosclerotic disease. This is because they are all people at high risk of CVD.
These three groups all require professional lifestyle and multifactorial risk factor management to defined lifestyle and risk factor targets.
9. Published Guidance: NICE For the primary prevention of CVD in primary care, a systematic strategy should be used to identify people aged 40�74 who are likely to be at high risk.
People should be prioritised on the basis of an estimate of their CVD risk before a full formal risk assessment. Their CVD risk should be estimated using CVD risk factors already recorded in primary care electronic medical records.
Risk equations should be used to assess CVD risk.
People should be offered information about their absolute risk of CVD and about the absolute benefits and harms of an intervention over a 10-year period.
10. Published Guidance: QOF Secondary prevention of coronary heart disease (CHD1-CHD14):
Records (Register)
Ongoing Management (Review)
Cardiovascular disease: Primary prevention (PP1-PP2)
Initial diagnosis (Risk Assessment)
Ongoing Management (Lifestyle advice)
11. The First Step
12. Meeting the Challenge Short, practical �how to� guide
Outlines existing guidance
Includes examples of good practice
Points to other sources of advice and information
13. Overview of Contents Introduction
About this guide
How to use it
Background
Rationale
Policy context
Establishing & Maintaining a Register
Defining & identifying those at �high risk�
Creating & validating a register
Risk assessment Managing People at High Risk of CVD
Communication of risk
Management of risk factors
Follow-up: Annual review
Training & competencies
Reaching the �hard to reach�
Levers/Incentives
Cost, capacity
Case studies
14. Purpose of Today Present the story so far
Identify & share good practice
Provide an opportunity to discuss issues & challenges (& reach a consensus on some)
Contribute to the development of the guide
10-15 mins to debate and discuss key questions under 3 headings
Record �consensus� and good practice examples (with contact details) on post-it notes and stick on relevant flip chart
We will summarise feedback at end
15. High CVD risk Definition-risk algorithm
Creating a register
Do we have adequate codes
Exclusion codes
Validating the register
Examples
16. Management of those at high CVD risk Annual review-suggested in the NHS Health Checks document
What should it include?
Recalculate risk?
Cholesterol?
Role of lifestyle interventions
Examples
17. Management of those at high CVD risk Pharmacological
Statins
Review
monitoring
Lifestyle interventions
Definition of adequate trial
�informed dissent�
Examples