Download
1 / 1
10 likes | 104 Views
Resources, Needs and Well-being of people with Multiple Sclerosis MacLurg K (1), Reilly P (1) Hawkins S (2); Evason E (3), Whittington D (3). 1. Department of General Practice, Queens University of Belfast. 2. Department of Neurology, Royal Victoria Hospital. 3. University of Ulster.

E N D
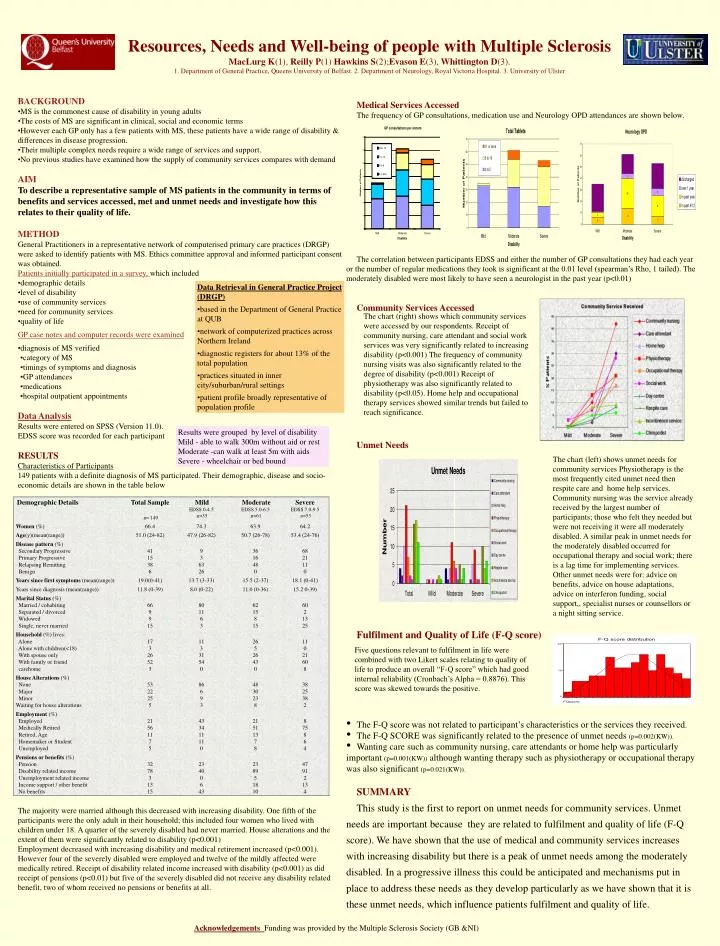
Resources, Needs and Well-being of people with Multiple SclerosisMacLurg K(1), Reilly P(1) Hawkins S(2);Evason E(3), Whittington D(3).1. Department of General Practice, Queens University of Belfast. 2. Department of Neurology, Royal Victoria Hospital. 3. University of Ulster • BACKGROUND • MS is the commonest cause of disability in young adults • The costs of MS are significant in clinical, social and economic terms • However each GP only has a few patients with MS, these patients have a wide range of disability & differences in disease progression. • Their multiple complex needs require a wide range of services and support. • No previous studies have examined how the supply of community services compares with demand • AIM • To describe a representative sample of MS patients in the community in terms of benefits and services accessed, met and unmet needs and investigate how this relates to their quality of life. • METHOD • General Practitioners in a representative network of computerised primary care practices (DRGP) were asked to identify patients with MS. Ethics committee approval and informed participant consent was obtained. • Patients initially participated in a survey, which included • demographic details • level of disability • use of community services • need for community services • quality of life • GP case notes and computer records were examined • diagnosis of MS verified • category of MS • timings of symptoms and diagnosis • GP attendances • medications • hospital outpatient appointments • Data Analysis • Results were entered on SPSS (Version 11.0). • EDSS score was recorded for each participant • RESULTS • Characteristics of Participants • 149 patients with a definite diagnosis of MS participated. Their demographic, disease and socio-economic details are shown in the table below • The majority were married although this decreased with increasing disability. One fifth of the participants were the only adult in their household; this included four women who lived with children under 18. A quarter of the severely disabled had never married. House alterations and the extent of them were significantly related to disability (p<0.001) • Employment decreased with increasing disability and medical retirement increased (p<0.001). However four of the severely disabled were employed and twelve of the mildly affected were medically retired. Receipt of disability related income increased with disability (p<0.001) as did receipt of pensions (p<0.01) but five of the severely disabled did not receive any disability related benefit, two of whom received no pensions or benefits at all. • Medical Services Accessed • The frequency of GP consultations, medication use and Neurology OPD attendances are shown below. • The correlation between participants EDSS and either the number of GP consultations they had each year or the number of regular medications they took is significant at the 0.01 level (spearman’s Rho, 1 tailed). The moderately disabled were most likely to have seen a neurologist in the past year (p<0.01) • Community Services Accessed • Unmet Needs • Fulfilment and Quality of Life (F-Q score) • The F-Q score was not related to participant’s characteristics or the services they received. • The F-Q SCORE was significantly related to the presence of unmet needs (p=0.002(KW)). • Wanting care such as community nursing, care attendants or home help was particularly important (p=0.001(KW)) although wanting therapy such as physiotherapy or occupational therapy was also significant (p=0.021(KW)). • SUMMARY • This study is the first to report on unmet needs for community services. Unmet needs are important because they are related to fulfilment and quality of life (F-Q score). We have shown that the use of medical and community services increases with increasing disability but there is a peak of unmet needs among the moderately disabled. In a progressive illness this could be anticipated and mechanisms put in place to address these needs as they develop particularly as we have shown that it is these unmet needs, which influence patients fulfilment and quality of life. • Data Retrieval in General Practice Project (DRGP) • based in the Department of General Practice at QUB • network of computerized practices across Northern Ireland • diagnostic registers for about 13% of the total population • practices situated in inner city/suburban/rural settings • patient profile broadly representative of population profile The chart (right) shows which community services were accessed by our respondents. Receipt of community nursing, care attendant and social work services was very significantly related to increasing disability (p<0.001) The frequency of community nursing visits was also significantly related to the degree of disability (p<0.001) Receipt of physiotherapy was also significantly related to disability (p<0.05). Home help and occupational therapy services showed similar trends but failed to reach significance. Results were grouped by level of disability Mild - able to walk 300m without aid or rest Moderate -can walk at least 5m with aids Severe - wheelchair or bed bound • The chart (left) shows unmet needs for community services Physiotherapy is the most frequently cited unmet need then respite care and home help services. Community nursing was the service already received by the largest number of participants; those who felt they needed but were not receiving it were all moderately disabled. A similar peak in unmet needs for the moderately disabled occurred for occupational therapy and social work; there is a lag time for implementing services. Other unmet needs were for: advice on benefits, advice on house adaptations, advice on interferon funding, social support,, specialist nurses or counsellors or a night sitting service. Five questions relevant to fulfilment in life were combined with two Likert scales relating to quality of life to produce an overall “F-Q score” which had good internal reliability (Cronbach’s Alpha = 0.8876). This score was skewed towards the positive. Acknowledgements Funding was provided by the Multiple Sclerosis Society (GB &NI)