Download
1 / 16
160 likes | 441 Views
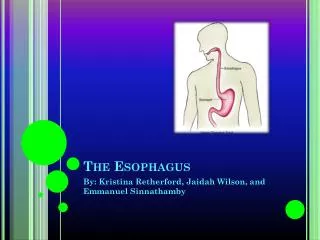
Surgical Management of Benign Esophagus. Scott Welle, DO, FACOS, FACS. Disclosure. Consultant Intuitive Surgical. Esophageal Anatomy. Esophagus lined by squamous epithelium except for distal 2 cm which is lined by columnar epithelium

E N D
Surgical Management of Benign Esophagus • Scott Welle, DO, FACOS, FACS
Disclosure • Consultant Intuitive Surgical
Esophageal Anatomy • Esophagus lined by squamous epithelium except for distal 2 cm which is lined by columnar epithelium • 3 areas of narrowing at cricopharyngeus, aortic arch, and diaphragm
Esophageal Anatomy • Vessels and Drainage • Arterial blood supply segmental from terminal sources • Lymphatic drainage extends longitudinally in the wall of esophagus before continuing to regional lymph nodes • Thoracic duct courses from right to left behind upper third of esophagus • Vagus nerves form a plexus on its musculature
Esophageal Anatomy • Gastroesophageal Junction • In humans no distinct anatomotic muscular sphincter • Presence of segment of esophagus exposed to intra-abdominal pressure most important anatomic consideration affecting the competence of the GE junction • In a sliding hiatal hernia the phrenoesophageal membrane is stretched • Anatomy of the phrenoesophageal membrane important factor in pathophysiology of GERD
Gastroesophageal Junction • In patients with reflux, attachment of phrenoesophageal ligament closer to stomach, intra-abdominal esophagus shorter • Two other important mechanisms in limiting exposure of distal esophagus to acid {1} esophageal clearing {2} proper gastric fuction
Gastric Reflux • Chronic destructive influences of reflux can produce metaplasia of normal squamous esophageal epithelium • Indications for surgery include symptoms or complications intractable to medical management • Medical management sufficient for majority of patients
Barrett’s Esophagus • Indications for anti-reflux surgery for Barrett’s not complicated by malignancy same as indications in any patient with GE reflux • Anti-reflux operations effective in relieving esophagitis • Any patient with Barrett’s esophagus requires careful follow-up with serial endoscopies and biopsy. If severe dysplasia esophageal resection is indicated. Severe dysplasia considered a Tis tumor
Hiatal Hernia • Type I ~ sliding hiatal hernia (most common) • Type II ~ classic paraesophageal hernia • Defect in phernoesophageal membrane • Type III ~ mixed paraesophageal • Type IV ~ giant hiatal hernia with other abdominal contents in chest ie colon, small intestine
Achalasia • Absence or degeneration of ganglia of Auerbach’s plexus. Manometrically absence of peristaltic waves • Esophagram may demonstrate “birds beak” narrowing of distal esophagus
Achalasia • Treatments • balloon dilation • botulism injection • Heller myotomy • Keys to heller • 2 cm myotomy on the stomach • 5 cm on esophagus • Often combined with partial fundoplication
Diverticula • True diverticula contain complete wall of mucosa, submucosa, muscle • False diverticula lack a muscular wall • In esophagus most are acquired • Pharyngoesophageal and epinephric are false diverticula
Diverticula • Pharyngoesophageal diverticulum (Zenker’s) lies posteriorly; all others usually lateral • Traction diverticula, true diverticula, caused by inflammation
Zenker treatment • Manometric findings often normal but may demonstrate incoodination • Cricopharyngotomy alone abolishes symptoms in most patients
Miscellanaus • Mallory-Weis tears - gastric bleeding that follows repeated emesis • Boerhaave’s syndrome - perforation and vomiting against a closed cardia
Benign esophageal tumors • Usually asympomatic • Leiomyomas most common benign esophageal lesions • Treatment simple enucleation