Download
1 / 79
940 likes | 1.8k Views
DISEASES OF THE ESOPHAGUS. Prof. Ferenc Szalay MD, PhD. 1st Department of Medicine of Semmelweis University Budapest, Hungary. Budapest, 03.02.2003 lecture for students. Diseases of the esophagus.

E N D
DISEASES OF THE ESOPHAGUS Prof. Ferenc Szalay MD, PhD 1st Department of Medicine of Semmelweis University Budapest, Hungary Budapest, 03.02.2003 lecture for students
Diseases of the esophagus GERDMotility disordersEsophagitis(infection, chemicals, pills)Neurological disordersSkeletal muscle disordersVaricesMallory-Weiss sy.Barrett’sTumors Common complainsWide range of symptoms
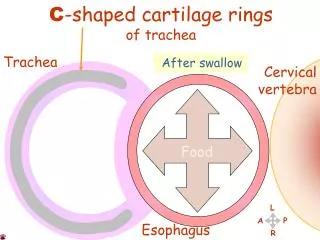
Swallowing Many muscle5 nerves : V, VII, IX, X, XIIStages oral - voluntary pharyngeal - involuntary esophageal - LES relaxed1 second 5 steps
5 steps within 1 second 1. Soft palate is elevated + retracted to prevent nasopharingeal reflux2. Vocal cords are closed Epiglottis swings backward closure the larynx3. UES relaxes4. Larynx is pulled upwardstreching, opening E and UES5. Contractions of pharyngeal muscle
Motility disorders of oropharynx • Dysfunction of the UES • Zenker’s diverticulum, Cricopharingeal bar • Neurologic disorders (stroke) • Cerebrovascular diseases, Poliomyelitis • Amyotrophic lateral sclerosis, Multiple sclerosis, Brain stem tumor • Skeletal musclular disorders • Myastenia gravis, Metabolic myopathy (T4 toxicosis, myxedema, steroid) • Muscular dystrophies • Local structural lesions • Neoplasms, extinsic compression (Thyroid, cervical spur), Surgery Common problem in the elderly patients and frequently associated with poor prognosis owing to a high incidence of aspiration
Motility disorders of the esophagus Smooth muscle diseases (scleroderma) Intrinsic nervous systemAchalasia, Chagas diseaseloss of ganglion cells in Auerbach plexus LES no peristalsisDiffuse esophagus spasm and its variants
Achalasia: Chagas’ disease Cause: Tripanosoma Cruzi inf.
Rings and Webs Schatzki’s ring- proximal or distal - congenital or secondary to GERDPlummer Vinson syndrome - upper E web - dysphagia - irondeficiency anemiaSymptoms if diameter < 13 mm - intermittent dysphagia for solid food - sudden: “steak house syndrome”Treatment - mechanical dilators
Post-mortem specimen from a similar case of esophageal narrowing in a young boxer.
AJCC Staging of Esophagus: TNM Staging Regional lymph nodes (N) Nx Regional lymph nodes cannot be assassed N0 No regional lymph node metastasis N1 Regional lymph node metastasis Distant metastasis (M) Mx Distant metastasis cannot be assassed M0 No distant metastasis M1 Distant metastasis Tumors of lower or upper esophagus M1a Metastasis in nonregional lymph node M1b Distant metastasis (eg: liver, bone, brain) Tumors of middle esophagus M1a Not applicable M1b Metastasis in nonregional lymph node or distant metastasis (eg: liver, bone, brain)
AJCC Staging of Esophagus: TNM Staging Stage Tumor Node Metastasis Stage 0 Tis N0 M0 Stage I T1 N0 M0 T2 N0 M0 Stage IIA T3 N0 M0 T1 N1 M0 Stage IIB T2 N1 M0 T3 N1 M0 Stage III T4 Any N M0 Stage IV Any T Any N M1 Stage IV A Any T Any N M1a Stage IV B Any T Any N M1b
INFECTIONS OF THE OESOPHAGUS Viral herpes, CMV Fungal Candida Most common in immuncompromized patients: AIDS Immunosuppressive treatment Immune defects Antibiotic os steroid treatment
Acid-related diseases of the oesophagus GERD / GORD
Definitions • Heartburn: • Burning retrosternal pain radiating upward due to exposure of the oesophagus to acid • Oesophagitis: • Endoscopically demonstrated damage to the oesophageal mucosa • Gastro-oesophageal reflux disease (GORD): • Pathological reflux ranges from simple to erosive to Barrett’s • Non-erosive reflux disease (NERD): • Reflux disease in which erosion does not occur Talley et al., BMJ 2001; 323: 1294–7. de Caestecker, BMJ 2001; 323: 736–9. Nathoo, Int J Clin Pract 2001; 55: 465–9. Quigley, Eur J Gastroenterol Hepatol 2001; 13(Suppl 1): S13–18.
bile reflux Pathophysiology of GORD salivary HCO3 Impaired mucosal defence oesophageal clearanceof acid (lying flat, alcohol, coffee) Impaired LOS(smoking, fat, alcohol) – transient LOS relaxations – basal tone Hiatus hernia acid output (smoking, coffee) H+ Pepsin Bile and pancreatic enzymes intragastric pressure(obesity, lying flat) gastric emptying(fat) de Caestecker, BMJ 2001; 323:736–9. Johanson, Am J Med 2000; 108(Suppl 4A): S99–103.
Diagnosis of GORD • History • 1. Does reflux exist? • 2. Is acid R responsible for symptoms? • 3. Has R led to esophagus damage? • Barium swallow • Radionuclide scintigraphy (99mTc sulfur colloid) • E. manometry • Bernstein test • pH monitoring • Endoscopy
Bernstein test Retrosternal pain for 0.1 N HCl
Los Angeles classification system for oesophagitis Grade A Grade B One or more mucosal breaks, no longer than 5 mm, that do not extend between the tops of two mucosal folds One or more mucosal breaks, more than 5 mm long, that do not extend between the tops of two mucosal folds Grade D Grade C One or more mucosal breaks, that are continuous between the tops of two or more mucosal folds, but which involve less than 75% of the circumference One or more mucosal breaks, that involve at least 75% ofthe oesophageal circumference Lundell et al., Gut 1999; 45: 172–80.
Savary-Miller classification of oesophagitis • Grade I • One or several erosions in one mucosal fold • Grade II • Several erosions in several mucosal folds, the erosions can merge • Grade III • Erosions surrounding the oesophageal circumference • Grade IV • Ulcer(s), strictures, shortening of the oesophagus • Grade V • Barrett’s epithelium Grade I - V Savary & Miller. The Esophagus. In: Handbook & Atlas of Endoscopy. Solothurn, Switzerland: Verlag Gassman AG, 1978: 119–205.
Grade I oesophagitis Savary-Miller classificationOne or several erosions in one mucosal fold Quigley, Eur J Gastroenterol Hepatol 2001; 13(Suppl 1): S13–18. Nathoo, Int J Clin Pract 2001; 55: 465–9. www.gastrolab.net
Grade II oesophagitis Savary-Miller classificationSeveral erosions in several mucosal folds, the erosions can merge www.gastrolab.net
Grade III oesophagitis Savary-Miller classificationErosions surrounding the oesophageal circumference Freytag et al., Atlas of gastrointestinal endoscopy. www.home.t-online.de/home/afreytag/indexe.htm
Grade IV oesophagitis Savary-Miller classificationUlcer(s), shortening of the oesophagus Freytag et al., Atlas of gastrointestinal endoscopy. www.home.t-online.de/home/afreytag/indexe.htm
Grade IV oesophagitis Savary-Miller classificationStricture Nadel, UCHC
Grade V oesophagitis Savary-Miller classificationModerate Barrett’s oesophagus Freytag et al., Atlas of gastrointestinal endoscopy. www.home.t-online.de/home/afreytag/indexe.htm
Grade V oesophagitis Savary-Miller classificationModerate Barrett’s oesophagus Chromoendoscopic picture Freytag et al., Atlas of gastrointestinal endoscopy. www.home.t-online.de/home/afreytag/indexe.htm
Barrett’s dysplasia Columnar cells instead of squamous cells
Grade V oesophagitis Savary-Miller classificationSevere Barrett’s oesophagus Freytag et al., Atlas of gastrointestinal endoscopy. www.home.t-online.de/home/afreytag/indexe.htm
Adenocarcinoma of the oesophagus Nadel/Saint Francis Hospital. In: Gastrointestinal Pathology. Fenoglio-Preiser, New York: Raven Press, 1989: 96–100.
Range of presentations of GORD Typical symptoms (Heartburn/regurgitation) Atypical symptoms Complications With oesophagitis Chest pain(visceral hyperalgesia) Oesophageal erosions and/or ulcers Without oesophagitis Stricture Hoarseness (‘reflux laryngitis’) Barrett’s oesophagus Asthma, chronic cough, wheezing Oesophageal adenocarcinoma Dental erosions Nathoo, Int J Clin Pract 2001; 55: 465–9.
Prevalence of heartburn or acid regurgitation % Women: at least weekly episodes Men: at least weekly episodes 40 Prevalence (%) 0 25–34 35–44 45–54 55–64 65–74 Age (years) Locke et al., Gastroenterology 1997; 112: 1448–56.
GORD can be a trigger for asthma 100 77 80 72 65 60 Asthma patients experiencing GORD symptoms (%) 40 20 0 Perrin-Fayolle et al. (n=150) O’Connell et al. (n=189) Field et al. (n=109) Harding & Sontag, Am J Gastroenterol 2000; 95(Suppl): S23–32.
Correlation of respiratory and oesophageal symptoms with oesophageal acid events Asthmatic patients with GORD (n=118) Wheezing or shortness of breath 65 Cough 98 Chest pain 60 Heartburn 83 Regurgitation 87 Nausea 91 0 20 40 60 80 100 Respiratory and oesophageal symptoms associated with oesophageal acid events (%) Harding et al., Chest 1999; 115: 654–9.