Download
1 / 69
690 likes | 736 Views
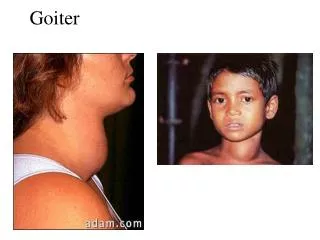
Goiter and Thyroid Cancer. Hasan AYDIN, MD Yeditepe University Medical Faculty Department of Endocrinology and Metabolism. Goiter. Definitions. Goiter is a diffuse or nodular enlargement of the thyroid gland resulting from excessive replication of benign thyroid epithelial cells.

E N D
Goiter and Thyroid Cancer Hasan AYDIN, MD Yeditepe University Medical Faculty Department of Endocrinology and Metabolism
Definitions Goiteris a diffuseornodularenlargement of thethyroidglandresultingfromexcessivereplication of benignthyroidepithelialcells. A thyroid noduleis a discrete lesion within the thyroid gland that is palpably and/or ultrasonog- raphically distinct from the surrounding thyroid parenchyma Incidentalomasarenon-palpablenodulesincidentallydiscovered on USG orotherradiologicalimagingperformedforotherreasons
Thyroid Function - Euthyroid - Hyperthyroid - Hypothyroid Structure - Diffuse - Nodular
Prevalence • Large population studies-Framingham study showed clinically significant nodules in 6.4% women and 1.5% men ages 30-59(total 4.2%) but thought to be significantly understated • Ultrasounds- 20% to 76% of females had at least one thyroid nodule on ultrasound • Autopsy surveys show 37 to 57% of patients with thyroid nodules
Rate of Carcinoma in Thyroid Nodules • Significant selection bias in surgical series • USA: Pts with nodules were referred to surgery without biopsy and 6.5% of excised nodules were carcinomas • Italy: 2327 pts with nodules were evaluated by FNA and of those 391 were selected for surgery. Carcinomas were found in 5% of total
Causes of Thyroid Nodules • Benign- >90% • Multinodular goiter (colloid adenoma) • Hashimoto’s (chronic lymphocytic) thyroiditis • Cysts: colloid, simple, or hemorrhagic-7-14% can be malignant- most commonly papillary ca with a cystic component with most increased size 2-4cm • Follicular Adenoma • Macrofollicular adenoma • Microfollicular or cellular • Hurthle-cell (oxyphil cell) adenomas- macro or microfollicular • Malignant -about 6% • Papillary • Follicular • Minimally or widely invasive • Oxyphilic type • Medullary • Anaplastic • Primary thyroid lymphoma • Metastatic carcinoma
Pathogenesis • Dyshormonogenesis or severe iodine deficiency • Impaired hormone synthesis • Secondarily and increase in TSH secretion. • TSH induces diffuse thyroid hyperplasia,followed by focal hyperplasia with necrosis and hemorrhage,finally the development of new areas of focal hyperplasia. • A clone of cells that may or may not be able to pick up iodine or synthesize thyroglobulin.
NODULAR GOITERPresentation • Asymptomatic • Neck mass discovered by patient or physician • Abnormal CXR • Symptomatic • Pressure symptoms • Hoarseness • Thyrotoxicosis
Whan a thyroidnodule is detected Malignant? Hyperfunctional? • Thyroid USG : Numberanddimentions of nodules • TSH and fT4
NODULAR GOITERSuspicious Nodule or Goiter • High suspicion • Family history of medullary thyroid carcinoma • Rapid tumor growth • A nodule that is very firm or hard • Fixation of the nodule to the adjacent structures • Paralysis of the vocal cord • Regional lymphadenopathy • Distant metastasis • Moderate suspicion • Age of either<20 or >70 years • Male sex • History of head and neck irradiation • A nodule >4 cm in diameter or partially cystic • Symptoms of compression, including dysphagia, dysphonia, hoarseness, dyspnea, and cough
NODULAR GOITEREvaluation • TSH • FT4, T3 • Radionuclide Scan/RAIU • US • CT Scan (without contrast) • FNA biopsy
Ultrasound • Provides considerable anatomic information but no functional information • Determine the volume of a nodule, multicentricity and whether it is cystic or solid- often performed before FNA • Extremely useful in also following patients being managed conservatively for possible increasing size of lesion • Unable, however, to accurately predict the diagnosis of solid nodules
Ultrasound • Cystic lesion are reassuring but only 1-5% of total thyroid nodules • In addition, as many as 25% of well-differentiated thyroid cancers had cystic components and up to 60-70% of all nodules • Physician can correlate the nuclear medicine and U/S finding and determine the function of the particular nodule • Additional nodules can be found 20-48% of patients • Many times the U/S findings differ from the physical exam, in one retrospective series up to 63% of the time
Ultrasound • Ultrasonographic Cancer Risk Factors for a Thyroid Nodule • hypoechogenicity, • microcalcifications, • irregular margins, • increased nodular flow visualized by Doppler, • the evidence of invasion or regional lymphadenopathy
NODULAR GOITERFNA Evaluation • Biopsy all accessible nodule(s) • Biopsy suspicious nodule(s) cold on scan; firm by palpation; growing in size • Results less reliable in large goiters • Most common diagnosis is “colloid nodule”
FNA • Simple, safe office procedure • Tissue sample obtained by 25 gauge needle • With experience adequate sample may be obtained in 90 -97% of aspirates of solid nodules • False negative rate (FNA benign but nodule turn out malignant) is 0-5% usually due to sampling error • False positive rates (malignant but turns out benign) <5% due to focal hyperplasia in a macrofollicular adenoma or cellular atypia in a degenerating adenoma
FNA results • Malignant- pt needs to have surgical management • Benign- observation with interval ultrasounds and clinical examinations • Indeterminate- radioisotope scan- perform suppression scan and if cold proceed to surgical management- if hot nodule consider observation • Non diagnostic-repeat FNA or U/S guided FNA
Functionality in ThyroidNodules TSH Hyperthyroid <0.5 mIU/ml Euthyroid 0.5-4 mIU/ml Hypothyroid >4 mIU/ml Thyroidscintigraphy
Imaging- Thyroid Scintigraphy • Utilizes iodine or technetium-99m pertechnate- more is taken up and organified by functional tissue • Non-functioning thyroid nodule is cold and mandates further work-up by FNA • The scan is often used in working up nodules in patients with low TSH levels • Only slightly more than one-half of the excised malignant thyroid nodules appear cold because the scan is 2-D there is apposition of normal thyroid tissue next to abnormal tissue
Also although 80% of nodules greater than 2cm appear cold- smaller nodules can be indeterminate • Malignancy has been shown to occur 15-20% of “cold” nodules and, additionally, in 5-9% of nodules with uptake that is “warm” or “hot” • Thyroid scintigraphy has fallen out of favor- definitely questions about how cost-effective it is for routine evaluation for patients with nodules
Thyroidnodule T USG TSH, T4 <1 cm No risk factor >1 cm orany risk factor Hyperthyroid Eutiroid Hypothyroid Tiroid scintigraphy Follow İİAB
II. Malignant Tumors A. Differentiated1. Papillary adenocarcinoma a. Pure papillary adenocarcinoma b.Mixed papillary and follicular ca (variants including tall cell, follicular, oxyphyl, solid) 2. Follicular adenocarcinomas (variants: "malignan adenoma", Hurthle cell carcinoma or oxyphil carcinoma, clear-cell carcinoma, insular carcinoma B.Medullary carcinoma- (not a tumor of follicular cells) C.Undifferentiated1. Small cell (to be differentiated from lymphoma) 2. Giant cell 3. Carcinosarcoma D.Miscellaneous 1. Lymphoma, sarcoma 2. Squamous cell epidermoidca 3. Fibrosarcoma 4. Mucoepithelial ca. 5. Metastatic tumor Neoplasms of the Thyroid (from WHO Classification) I. AdenomasA. Follicular 1. Colloid variant 2. Embryonal 3. Fetal 4. Hurthle cell variant B. Papillary (probably malignant) C. Teratoma
THYROID CANCER • Papillary (mixed papillary and follicular)75% • Follicular carcinoma 16% • Medullary carcinoma 5% • Undifferentiated carcinomas 3% • Miscellaneous (lymphoma, fibrosarcoma, 1% squamous cell carcinoma, malignant hemangioendothelioma, teratomas, and metastatic carcinomas)
Medullary Carcinoma Miscellaneous Sarcoma Lymphoma Squamous cell carcinoma Mucoepidermoid carcinoma Clear cell tumors Pasma cell tumors Metastatic Direct extention Kidney Colon Melanoma Classification of Malignant Thyroid Neoplasms • Papillary carcinoma • Follicular variant • Tall cell • Diffuse sclerosing • Encapsulated • Follicular carcinoma • Overtly invasive • Minimally invasive • Hurthle cell carcinoma • Anaplastic carcinoma • Giant cell • Small cell
Well-Differentiated Thyroid Carcinomas (WDTC) - Papillary, Follicular, and Hurthle cell • Pathogenesis - unknown • Papillary has been associated with the RET proto-oncogene but no definitive link has been proven (Geopfert, 1998) • Certain clinical factors increase the likelihood of developing thyroid cancer • Irradiation - papillary carcinoma • Prolonged elevation of TSH (iodine deficiency) - follicular carcinoma (Goldman, 1996) • relationship not seen with papillary carcinoma • mechanism is not known
WDTC - Papillary Carcinoma • 60%-80% of all thyroid cancers (Geopfert, 1998, Merino, 1991) • Histologic subtypes • Follicular variant • Tall cell • Columnar cell • Diffuse sclerosing • Encapsulated • Prognosis is 80% survival at 10 years (Goldman, 1996) • Females > Males • Mean age of 35 years (Mazzaferri, 1994)
WDTC - Papillary Carcinoma(continued…) • Lymph node involvement is common • Major route of metastasis is lymphatic • 46%-90% of patients have lymph node involvement (Goepfert, 1998, Scheumann, 1984, De Jong, 1993) • Clinically undetectable lymph node involvement does not worsen prognosis (Harwood, 1978)
WDTC - Papillary Carcinoma (Continued…) • Microcarcinomas - a manifestation of papillary carcinoma • Definition - papillary carcinoms smaller than 1.0 cm • Most are found incidentally at autopsy • Autopsy reports indicate that these may be present in up to 35% of the population (Mazzaferri, 1993) • Usually clinically silent • Most agree that the morbidity and mortality from microcarcinoma is minimal and near that of the normal population • One study showed a 1.3% mortality rate (Hay, 1990)
WDTC - Papillary Carcinoma(continued…) • Pathology • Gross - vary considerably in size - often multi-focal - unencapsulated but often have a pseudocapsule • Histology - closely packed papillae with little colloid - psammoma bodies - nuclei are oval or elongated, pale staining with ground glass appearanc - Orphan Annie cells
WDTC - Follicular Carcinoma • 20% of all thyroid malignancies • Women > Men (2:1 - 4:1) (Davis, 1992, De Souza, 1993) • Mean age of 39 years (Mazzaferri, 1994) • Prognosis - 60% survive to 10 years (Geopfert, 1994) • Metastasis - angioinvasion and hematogenous spread • 15% present with distant metastases to bone and lung • Lymphatic involvement is seen in 13% (Goldman, 1996)
WDTC - Follicular Carcinoma(Continued…) • Pathology • Gross - encapsulated, solitary • Histology - very well-differentiated (distinction between follicular adenoma and carcinomaid difficult) - Definitive diagnosis - evidence of vascular and capsular invasion • FNA and frozen section cannot accurately distinquish between benign and malignant lesions
WDTC - Hurthle Cell Carcinoma • Variant of follicular carcinoma • First described by Askanazy • “Large, polygonal, eosinophilic thyroid follicular cells with abundant granular cytoplasm and numerous mitochondria” (Goldman, 1996) • Definition (Hurthle cell neoplasm) - an encapsulated group of follicular cells with at least a 75% Hurthle cell component • Carcinoma requires evidence of vascular and capsular invasion • 4%-10% of all thyroid malignancies (Sessions, 1993)
WDTC - Hurthle Cell Carcinoma(Continued…) • Women > Men • Lymphatic spread seen in 30% of patients (Goldman, 1996) • Distant metastases to bone and lung is seen in 15% at the time of presentation
WDTC - Prognosis • Based on age, sex, and findings at the time of surgery (Geopfert, 1998) • Several prognostic schemes represented by acronyms have been developed by different groups: • AMES (Lahey Clinic, Burlington, MA) • GAMES (Memorial Sloan-Kettering Cancer Center, New York, NT) • AGES (Mayo Clinic, Rochester, MN)
WDTC - Prognosis (Continued…) • Depending on variables, patients are categorized in to one of the following three groups: 1) Low risk group - men younger than 40 years and women younger than 50 years regardless of histologic type - recurrence rate -11% - death rate - 4% (Cady and Rossi, 1988)
WDTC - Prognosis (Continued…) • 1) Intermediate risk group - Men older than 40 years and women older than 50 years who have papillary carcinoma - recurrence rate - 29% - death rate - 21% • 2) High risk group - Men older than 40 years and women older than 50 years who have follicular carcinoma - recurrence rate - 40% - death rate - 36%
Medullary Thyroid Carcinoma • 10% of all thyroid malignancies • 1000 new cases in the U.S. each year • Arises from the parafollicular cell or C-cells of the thyroid gland • derivatives of neural crest cells of the branchial arches • secrete calcitonin which plays a role in calcium metabolism
Medullary Thyroid Carcinoma (Continued…) • Developes in 4 clinical settings: • Sporadic MTC (SMTC) • Familial MTC (FMTC) • Multiple endocrine neoplasia IIa (MEN IIa) • Multiple endocrine neoplasia IIb (MEN IIb)
Medullary Thyroid Carcinoma (continued…) • Sporadic MTC: • 70%-80% of all MTCs (Colson, 1993, Marzano, 1995) • Mean age of 50 years (Russell, 1983) • 75% 15 year survival (Alexander, 1991) • Unilateral and Unifocal (70%) • Slightly more aggressive than FMTC and MEN IIa • 74% have extrathyroid involvement at presentation (Russell, 1983)
Medullary Thyroid Carcinoma (Continued…) • Familial MTC: • Autosomal dominant transmission • Not associated with any other endocrinopathies • Mean age of 43 • Multifocal and bilateral • Has the best prognosis of all types of MTC • 100% 15 year survival (Farndon, 1986)