Download
1 / 56
650 likes | 1.31k Views
Thyroid Cancer. May 10, 2006. Thyroid Cancer. Accounts for 1.5% of all cancers in the US Most common endocrine malignancy (95%) 22,000 cases per year and estimated 500 – 1000 patients die annually 90% of thyroid cancer cases have favorable prognosis.

E N D
Thyroid Cancer May 10, 2006
Thyroid Cancer • Accounts for 1.5% of all cancers in the US • Most common endocrine malignancy (95%) • 22,000 cases per year and estimated 500 – 1000 patients die annually • 90% of thyroid cancer cases have favorable prognosis
Classification & Incidence of Thyroid Cancer Follicular cell origin • Differentiated • Papillary 80% • Follicular 10% • Hurthle cell 3-5% • Undifferentiated • Anaplastic 1-2% Parafollicular cell origin – Medullary 5%
Papillary Carcinoma • Accounts for 90% radiation induced cancer • Classified as microcarcinoma, intrathyroidal, and extrathyroidal • Histologic variants: tall-cell, clear-cell, columnar, diffuse sclerosing • Multicentric in 30-50% of tumors • Spreads via lymphatics with propensity for mid- and lower-anterior cervical chain (Level VI) • 20-50% patients have involvement of cervical LN
Follicular Carcinoma • Only 10% of thyroid cancers in developed countries, although more prevalent in regions with iodine deficiency • Diagnosis depends on demonstration of vascular or capsular invasion • Classified as minimally or widely invasive • Vascular invasion tends to have a more aggressive course than capsular invasion • Uncommon to have multicentric disease • Hematogenous spread
Follicular Carcinoma Where does follicular carcinoma tend to metastasize? • Bone • Lung
Hurthle Cell Carcinoma • High propensity to spread to cervical lymph nodes and high incidence of distant metastasis • Less than 10% of Hurthle cell carcinomas take up radioiodine • High tumor recurrence rate • High mortality rate – 30% mortality at 10 years
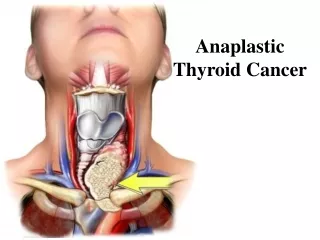
Anaplastic Carcinoma • Increasingly rare • Arise within differentiated cancers • Pts > 60 years old with rapidly expanding neck mass • Local invasion very common at time of dx (FNA) • Surgery plays limited role given advanced stage at dx • Radiation and chemotherapy have not demonstrated any significant improvement in survival • Median survival ~ 4 - 6 months
Medullary Thyroid Carcinoma • Originates from the parafollicular C cells • Elevation in calcitonin and CEA (50%) • 80% have sporadic MTC (unifocal), remainder have genetic component • 75% patients have LN metastasis at time of dx, 20% distant mets
Medullary Thyroid Carcinoma • MEN IIA • MTC (100%), pheo (40%), hyperparathyroidism (35%) • AD inheritance • Missense mutation of extracellular cysteine of RET • Surgery recommended before 6 years of age • MEN IIB • MTC (100%), pheo (50%), mucosal ganglioneuromas (100%), marfanoid habitus • AD inheritance • Missense mutation of tyrosine kinase domain of RET • Surgery recommended in infancy • Familial MTC
Lymphoma of the Thyroid • Usually non-Hodgkin’s B cell type • Pts with Hashimoto’s thyroiditis have 70-80 fold increase risk • Typically women > 70yo present with enlarging neck mass • FNA > 80% accuracy • Treatment includes XRT and chemotherapy • 5 year survival rates 50-70%
45 year old female presents to your office with a thyroid nodule. What questions will you ask her?
History • Characteristics of nodule • Is the patient symptomatic? • Hyperthyroid/Hypothyroid • Compressive sxs • Family history MEN endocrinopathies • Radiation exposure
45 year old female with thyroid nodule • Characteristics of nodule found incidentally by PCP • Is the patient symptomatic? No • Hyperthyroid/Hypothyroid • Compressive sxs • Family history None • Radiation exposure None
Physical Exam • Size • Consistency of nodule, multiple or solitary • Fixed or mobile • Presence of cervical LAD
Physical Exam • Solitary nodule • Mobile, not obviously adherent to adjacent structures • No cervical LAD • Normal voice • Otherwise well appearing
Evaluating a thyroid nodule • Thyroid nodules are common, but less than 10% are malignant • History and PE • TSH level should be obtained during initial evaluation • If low, radioisotope study • If normal or high, then proceed to ultrasound
Evaluating a thyroid nodule What is the risk of a “hot” nodule on radioiodine scan being malignant? • Less than 1% What about a “cold” nodule? • 15% – 20%
Evaluating a thyroid nodule • Radioisotope studies may also be useful: • FNA reports “suspicious for follicular neoplasm” or “indeterminate” • Detecting neck metastasis
Evaluating a thyroid nodule • What information will an ultrasound provide? • Number of nodules • Location and size of nodules • Cystic versus solid
Evaluating a thyroid nodule • Which of the following are concerning findings on ultrasound? • Halo sign • Hypoechogenic • Calcifications • < 1cm
Evaluating a thyroid nodule • Which of the following are concerning findings on ultrasound? • Halo sign • Hypoechogenic • Calcifications • < 1cm
Evaluating a thyroid nodule • FNA is the most reliable and cost efficient way to determine malignant from benign lesion • 4 categories: • Malignant, benign, suspicious, indeterminate • Limitation of FNA: • Cannot distinguish benign follicular or Hurthle cell adenoma from malignancy – based upon presence or absence of capsular or vascular invasion • False negative rate < 5%
45 year old female with thyroid nodule • TSH level was normal • Underwent an ultrasound-guided FNA of the nodule, pathology revealed papillary carcinoma in a nodule measuring 2.5cm
Management of Papillary Carcinoma What surgical procedure would you offer her? • Near-total or total thyroidectomy is recommended if: • Tumor > 1-1.5cm • Contralateral nodules • Local or regional metastasis • + FHx in 1st degree relative • + history of radiation exposure • Age >45 yo • Increased extent of surgery lowers recurrence rates and has improved survival in high-risk patients
Management of Papillary Cancer When is lobectomy an acceptable surgical procedure for FNA proven papillary cancer? • According to the American Thyroid Association Guidelines Taskforce, lobectomy with isthmusectomy may be sufficient treatment for microcarcinoma ( 1cm), low-risk patients, intrathyroidal cancer without involvement of cervical LN
Management of Papillary Cancer Will you plan on performing a lymph node dissection? • A central compartment (Level VI) neck dissection should be considered • If nodal disease is evident clinically then a more extensive cervical lymphadenectomy should be performed • LN sampling not recommended
Surgical Anatomy:Lymphatics • What are the LNs located superior to the thryoid gland in the midline called? • Delphian nodes
45 year old female with papillary carcinoma Patient opted to have a total thyroidectomy and surgical specimen demonstrated unifocal disease with capsular invasion and negative LN. Does she have a favorable or unfavorable prognosis?
Prognostic Risk Classification for Patients with Well-Differentiated Thyroid Cancer (AMES or AGES) Low Risk High Risk • Age <40 years >40 years • Sex Female Male • Extent No local extension, Capsular invasion, extra- intrathyroid, no caps thyroidal extension invasion • Metastasis None Regional/distant • Size <2 cm >4 cm • Grade Well diff Poorly diff
Management of Papillary Cancer What further treatment is recommended? • TSH suppression therapy • Radioiodine ablation therapy
45 year old female with papillary carcinoma She wants to know what her long-term survival is. What will you tell her? • ~ 90% at 10 years for papillary carcinoma
45 year old female with thyroid nodule • TSH level was normal • Underwent an ultrasound-guided FNA of the nodule, pathology suspicious for a follicular neoplasm • What is the risk that this is malignant? • Approximately 20% • What surgical procedure will you offer her?
Management of FNA suspicious for follicular neoplasm • Lobectomy would be a reasonable surgical procedure, particularly in low-risk patient who prefers limited surgical intervention • Near-total or total thyroidectomy still recommended for high-risk patient and/or large tumor size
Management of FNA suspicious for follicular neoplasm • Intra-operative frozen sections can be helpful in this scenario? True or false • False
45 year old female with thyroid nodule • You performed a lobectomy and the final pathology reveals Hurthle cell carcinoma • What further treatment do you recommend? • Completion thyroidectomy with central compartment LN dissection • TSH suppression therapy
Post-operative radioiodine remnant ablation • To whom should it be offered? • Stages III and IV disease • Stage II disease in pts under age 45 • Selected pts with Stage I • Multifocal disease • Nodal metastasis • Extrathyroidal extension • Vascular invasion • Aggressive histology
T1 2cm T2 2-4cm T3 >4cm, limited to thyroid T4a Any size, invasion of SQ, trachea, esophagus, RLN T4b Any size invasion of prevertebral fascia or encasing carotid/mediastinal vessels N0 no nodes N1a Level VI N1b All other levels Stages Stage I T1, N0, M0 Stage II T2, N0, M0 Stage III T3, N0, M0 T1-3, N1a, M0 Stage IVA T4a, N0, M0 T4a, N1a, M0 T1-3, N1b, M0 Stage IVB T4b, any N, M0 Stage IVC Any T and N, M1 TMN Classification for differentiated thyroid cancer
45 year old female with thyroid nodule She asks what her overall 10 year survival will be with her diagnosis of Hurthle cell carcinoma? • ~70% What if she had follicular carcinoma? • ~70%
Recommendations for follow-up(differentiated cancers) • Thyroid cancer recurs in 20-40% patients, most commonly within the first 2 years • Thyroglobulin used as tumor marker checked every 6-12 months • Whole body scan may be useful in intermediate and high-risk patients 6-12 months after ablation • Ultrasound should be done 6-12 months after surgery, then annually for the next 3-5 years
Management of recurrent and metastatic disease • Surgery mainstay of treatment for locoregional disease radioiodine radiation • Metastatic disease treated with radioiodine • Older patients with bony mets are less likely to respond to radioiodine and have poor prognosis • Pulm mets more radio responsive than bone mets
55 year old male presents to your office with MTC on FNA • Palpable thyroid nodule and cervical LN • Diarrhea and flushing • No FHx of MEN endocrinopathies • Calcitonin elevated, FNA reveals MTC Any further tests that you should order? • Genetic testing • CT scan to see extent of disease
55 year old male presents to your office with MTC on FNA What surgical procedure will you recommend to him? • Total thyroidectomy with LN dissection in Level VI and LN sampling in lateral regions (frozen sectioning intra-operatively)
55 year old male presents to your office with MTC on FNA What do you want to check for before bringing him into the operating room? • Presence of a pheochromocytoma
55 year old male presents to your office with MTC on FNA How would you handle the parathyroid glands? • Some recommend performing a total parathyroidectomy with autotransplantation in either the forearm or SCM
55 year old male presents to your office with MTC on FNA • Further treatment remains controversial but includes radiation therapy and chemotherapy • Surveillance using calcitonin levels
Surgical Anatomy What is the consequence of injurying the external branch of the superior laryngeal nerve? • Injury results in paralysis of the cricothyroid muscle