Download
1 / 40
400 likes | 438 Views
Leukemias. Normal myelopoiesis. Definition of leukemias:. The leukaemias are a group of disorders characterized by the accumulation of malignant white cells in the bone marrow and blood. These abnormal cells cause symptoms because of: (i) bone marrow failure

E N D
Definition of leukemias: The leukaemias are a group of disorders characterized by the accumulation of malignant white cells in the bone marrow and blood. These abnormal cells cause symptoms because of: (i) bone marrow failure (i.e. anaemia, neutropenia, thrombocytopenia) and (ii) infiltration of organs (e.g. liver, spleen, lymph nodes, meninges, brain, skin or testes).
The nature of leukaemia Leukaemia is a disease resulting from the neoplastic proliferation of haemopoietic or lymphoid cells. It results from mutation of a single stem cell, the progeny of which form a clone of leukaemic cells.Usually there is a series of genetic alterations rather than a single event. resulting in: (i) an increased rate of proliferation; (ii) reduced apoptosis and (iii) a block in cellular differentiation.
Leukaemias are broadly divided into: acute leukaemias, which, if untreated, lead to death in weeks or months chronic leukaemias, which, if untreated, lead to death in months or years
They are further divided into: lymphoid myeloid mixed lineage (biphenotypic or bilineage) leukaemias, showing usually both lymphoid and myeloid differentiation
Classification of leukemias: Acute leukemias: - Acute myeloblastic leukemias Acute lymphoblastic leukemias- Chronic leukemias Chronic myeloid (granulocytic) leukemias (CML)- -Chronic lymphocytic leukemias (CLL) -Other Chronic lymphoid leukemias (Hairy cell leukemias, prolymphocytic leukemia, lymphoma/leukemia syndrome)
classification The FAB classification based on morphology supplemented by cytochemistry and to some extent by immunophenotyping. Over the last decade the FAB classification has been increasingly supplemented or replaced by the WorldHealth Organization (WHO) Classification of Tumoursof Haematopoietic and Lymphoid Tissues
Classification of AML according to FAB group French-American-British classification
Classification of AML according to FAB group French-American-British classification
The FAB classification of ALL L1: blast cells are small, uniform, high nuclear to cytoplasmic ratio. L2: blast cells are large, heterogeneous, lower nuclear to cytoplasmic ratio. L3: vaculated blast, basophilic cytoplasm (usually B- ALL)
WHO proposed classification of acute lymphoblastic leukemia Precursor B lymphoblastic leukemia / lymphoblastic lymphoma:● ALL with t(9;22)(q34;q11.2); BCR-ABL (Philadelphia chromosome)● ALL with t(v;11q23) (MLL rearranged)● ALL with t(1;19)(q23;p13.3); TCF3-PBX1 (E2A-PBX1)● ALL with t(12;21)(p13;q22); ETV6-RUNX1 (TEL-AML1)● Hyperdiploid > 50● Hypodiploid● t(5;14)(q31;q32); IL3-IGHPrecursor T lymphoblastic leukemia / lymphoma
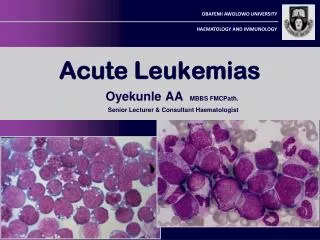
Pathogenesis of AL Acute leukaemias are characterized by a defect in maturation ,leading to an imbalance between proliferation and maturation; since cells of the leukaemic clone continue to proliferate without maturing to end cells ,there is continued expansion of the leukaemic clone and immature cells predominate. Their accumulation result in replacement of normal hemopoietic precursor cells of BM by myeloblast or lymphoblast & ultimately in BM failure Peripheral blood involvement & infiltration of organs occur Chronic leukaemias are characterized by an expanded pool of proliferating cells that retain their capacity to differentiate to end cells
Epidemiology of AL AL comprise 50 % of leukemia in clinical practice Leukaemia is the most common childhood cancer and acute lymphoblastic leukaemia (ALL) is the most common subtype, accounting for 75 – 80% of all cases. ALL is common in children (3-4y) failing off by 10 y, 2nd rise after 40 y Acute myeloid leukaemia (AML) has an incidence of 2 – 3 per100 000 per annum in children, rising to 15 per 100 000 in older adults. It can occur at all ages but has its peak incidence in the seventh decade
Diagnosing acute leukaemia The diagnosis of acute leukaemia usually starts from a clinical suspicion. It is uncommon for this diagnosis to be incidental, resulting from the performance of a blood count for a quite different reason. Clinical features suspicion of acute leukaemia blood count and film being performed and, if this shows a relevant abnormality, bone marrow aspiration. The diagnosis then rests on an assessment of the peripheral blood and bone marrow.
Clinical features Due to BM failure 1- pallor, lethargy & dyspnoea from anemia. 2- Fever , malaise , feature of mouth, throat, respiratory, perianal or other infections including septicemia , are common 3- spontaneous bruises , purpura bleeding gum, menorrhagia &bleeding from venepuncture sites because of thrombocytopenia are common . Occasionally there is major internal bleeding. A bleeding tendency due to thrombocytopenia & DIC is characteristic of M3
Due to organ infiltration 1- Tender bones especially in children 2- superfacial lymphadenopathy in ALL 3-Moderate splenomegaly, hepatomegaly especially in ALL 4- Gum hypertrophy & infiltration, skin involvement in M4&M5 lysosomal released from blast may cause renal damage & K loss & hypokalemia inM5 5- meningeal syndrome particularly in ALL & rarely in AML M4 & M5 , headache, nausea & vomiting, blurring of vision & diplopia 6- other manifestations like testicular swelling in ALL or singe of mediastinal compression in T-ALL
Lab. Findings Hematological investigation may reveal the following: 1- Normochromic normocytic anemia 2- Total WBC count may be decreased, normal or increased 3- Thrombocytopenia is most often extreme in AML
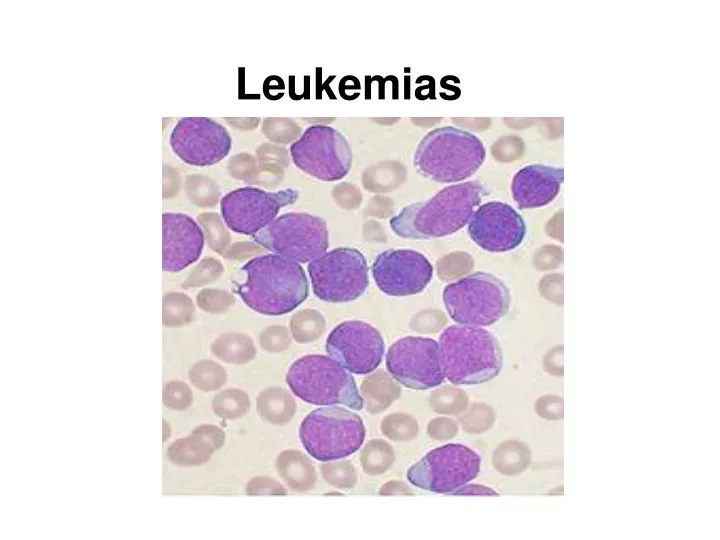
4- Blood film examination typically show number of blast cells in AML the blast may contain aure rods & other abnormal cells may present e.g. promyelocyte, myelocyte,agranular neutrophils,pseudo-pelger cells or myelocytic cells .In M6 (erythroleukemia) many erythroblast may be found.
5-The BM is hypercellular with marked proliferation of leuk. Blast cells ≥ 50% & typically more than 75% of total BM cells. in ALL the marrow is difficult to aspirate because of increased reticulin fibers. In M7 the patient typically has acute onset of pancytopenia with BM fibrosis.
Other investigations *Test for DIC are positive in patient with M3 *Lumber puncture show that spinal fluid has an increased pressure & contain leuk. cells in patient with meningeal leuk. • *X-ray may reveal lytic bone lesion especially in children ALL , A mediastinal mass of thymus &/or lymph nodes is characteristic of T-ALL ,& infiltration of lung due to infection or less frequently due to leuk. itself *Biochemical tests may reveal raised serum uric acid, serum lactic dehydrogenase & less commonly hypercalcemia Liver & renal function tests performed as baseline before treatment.
Special tests includes: -Cytochemistry: this may help to show granule development or monocytic differentiation in AML & help to distinguish ALL subtypes The myeloperoxidase or Sudan black reactions are most useful in establishing the identity of AML and distinguishing from ALL. The non-specific esterase stain is used to identify a monocytic component in AMLs and to distinguish a poorly differentiated monoblastic leukemia from ALL
- Immunological markers: used to distinguish AML from ALL & are particularly useful in sub- classifying ALL.
Special tests includes: - Immunoglobulin & T-cell receptor gene rearrangements: is sensitive method for detection of monoclonal population of B or T cells in ALL & occasionally in AML. - Chromosomal analysis: certain chromosomal changes are typical of different sub types of AML &ALL. They are useful in diagnosis &monitoring of residual disease during therapy & may carry prognostic significance e.g. : Ph + ALL has poor prognosis Hyperdiploidy in ALL is good prognostic feature
Hybrid acute leuk. In minority of cases of AL, the blast cells on special testing show features of both ALL & AML. These features may be on the same cell (biphenotypic) or on separate population (bilinear).They include inappropriate expression of immunological markers or inappropriate gene rearrangement.