Download
1 / 27
280 likes | 454 Views
Chronic leukemias. Chronic leukemias. Chronic myelogenous (granulocytic) leukemia Is characterized by an unregulated proliferation of myeloid elements in the bone marrow, liver and spleen, leading to marked leukocytosis and organomegaly. Incidence 20% of all leukemias

E N D
Chronic leukemias • Chronic myelogenous (granulocytic) leukemia • Is characterized by an unregulated proliferation of myeloid elements in the bone marrow, liver and spleen, leading to marked leukocytosis and organomegaly. • Incidence • 20% of all leukemias • Primarily affects adults 25-60 years old, with a peak incidence at 40-59. • Etiology, pathogenesis and physiology • May occur after anything that can induce chromosomal aberrations such as ionizing radiation, alkylating agents, and exposure to other biologically active chemicals
Chronic leukemias • Appears to be a clonal hematopoietic stem cell disorder • 90% of CML have a Philadelphia (Ph’) chromosome (reciprocal translocation between chromosome 22 and chromosome 9by cytogenetic karyotype studies. • A BCR/ABL hybrid gene is created when the breakpoint is in the major breakpoint cluster region of chromosome 22. The gene product (p290) has enhanced tyrosine kinase activity that results in • Increased granulocyte-colony stimulating factor • Increased platlet derived growth factor • Suppression of apoptosis in hematopoietic cells • The remaining 5-10% are positive for the translocation using more sensitive DNA studies such as RT-PCR or fluorescent in situ hybridization • The Ph’ chromosome is found in all hematopoietic cells except T lymphocytes (and sometimes B lymphocytes) • The Ph’ cells have a growth advantage over normal cells
Chronic leukemias • The progeny of the original malignant cell, after 2-6 years, eventually replace the normal hematopoietic elements and become the prominent cell • By the time the disease becomes clinically evident, nearly all the myeloid cells in the bone marrow are Ph’ + • As the disease progresses, the Ph’ + cells undergo additional chromosomal aberrations and the patients ultimately terminate in a blast crisis. • Note - A Philadelphia chromosome generated by a break in the minor breakpoint region of chromosome 22 resulting in a fusion protein product, p190, may be seen in AML. • The clinical course of the disease occurs in three stages • Asymptomatic, proliferative stage – Ph’+ cells appear in the bone marrow and the peripheral leukocyte count is normal
Chronic leukemias • The symptomatic, chronic stage occurs after about 6.3 years – at this stage the peripheral leukocyte count is increased and immature granulocytes appear in the peripheral blood. • The hyperproliferation is easily controlled with chemotherapy, but the remission is only temporary and patients still have Ph’+ cells in the bone marrow. • Accelerated or acute stage – this is also called a blast crisis (>30% blasts in the bone marrow) • Cellular proliferation is uncontrollable and resembles AML. • The medium survival is 10 weeks • Signs and symptoms • Malaise • Fatigue due to anemia • Fever
Chronic leukemias • Weight loss • Sweating • Bone aches and fullness in upper abdomen due to expansion of the bone marrow and organomegaly • Bleeding, petechiae, ecchymoses from abnormal platlets • Lab features • Leukocytosis and anemia; ¾ have WBC counts> 100 x 109/L • Normal appearing granulocytes at all stages of maturation are seen in the peripheral smear (they are not functionally normal, however); < 10% are blasts and promyelocytes • Many have a thrombocytosis with variation in shape; platlet function is frequently abnormal • Low to absent leukocyte alkaline phosphatase activity (Low LAP score)
Chronic leukemias • Treatment • Median survival from the time of diagnosis used to be ~ 3 years • The prognosis is better if the WBC count is lower and the % of blasts is low • Chemotherapy with a single agent has been used and ~ 75% in the chronic phase of the disease go into remission. However, Ph’+ cells remain in the bone marrow • Bone marrow transplants during the chronic phase (high dose chemo/radiotherapy followed by infusion of normal, compatible bone marrow) used to be the best therapy • A new drug, Gleevec, is now available and it specifically targets the BCR/ABL gene product. The Ph’ + cells are destroyed, while normal cells are unaffected
Chronic leukemias • Eosinophilic leukemia • Is this a distinct entity or a variant of CML? • 30-70% eosinophils with a WBC count > 30 x 109/L and a shift to the left • The prognosis is poor with a median survival of < 1 year • Basophilic leukemia • Is this a distinct entity or a variant of CML? • Is extremely rare with 40-80% basophils and a left shift
Chronic leukemias • Chronic lymphocytic leukemia • This is predominantly a disease of the elderly; > 90% are over 50 and 2/3 are over 60; male:female is 2:1 • Is characterized by peripheral and bone marrow lymphocytosis and a survival of a few years to > 10 years • This is a B cell abnormality • The lymphocytes appear normal, but are immunologically incompetent. However, some functionally normal B cells remain and there is a normal T cell pool
Chronic leukemias • Etiology • Genetic factors are important since it runs in families • Clinical course • The pace of the disease varies and is dependent on the rate of accumulation of abnormal lymphocytes • Median survival is 3-4 years, but 10-15% survive > 10years • There is no tendency for blast transformation, but complications of advanced disease result from progressive accumulation of long-lived, poorly functional lymphocytes. • Signs and symptoms • Organomegaly and lymphadenopathy • Often discovered accidentally • Fatigue
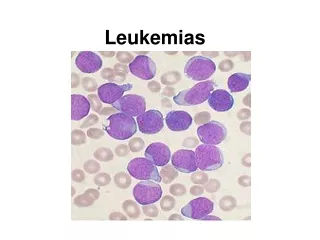
Chronic leukemias • Near the end – bruising, pallor, fever, and weight loss • Lab features • Absolute lymphocytosis of 10-150 x 109/L • Lymphocytes usually appear normal, but they are markedly fragile and smudge cells are seen on the peripheral smear • It is not necessary to do a bone marrow biopsy for diagnosis. • Anemia occurs late in the disease and may be due to decreased production secondary to marrow infiltration, hypersplenism, or autoimmune hemolytic anemia: the same things may cause neutropenia or thrombocytopenia • Hypogammaglobulinemia as the disease progresses
CLL with smudge cells Smudge cell
Chronic leukemias • Prognosis is related to the extent and distribution of the disease – also called the stage: • Stage A – lymphocytosis without anemia or thrombocytopenia and < 3 areas of lymphoid involvement (lymph nodes, spleen, liver) • Stage B – same as A, but > 3 areas of lymphoid involvement • Stage C – lymphocytosis with anemia, thrombocytopenia, or both
Chronic leukemias • Treatment • Stage A – observe only • Stage B with no symptoms – same as A • Stage B with symptoms - therapeutic intervention to relieve signs and symptoms • Stage C - therapeutic intervention to relieve signs and symptoms • The goal of therapy is simply to relieve signs and symptoms • A new monoclonal antibody, CAMPATH, that targets the mature B cells in B cell CLL is now being used.
Chronic leukemias • Differential diagnosis • Must distinguish between CLL and prolymphocytic leukemia, hairy cell leukemia, large, granular lymphocyte leukemia, Sezary’s syndrome, and circulating lymphoma cells • Prolymphocyte leukemia • This is an aggressive leukemic disorder of mature B or T cells • > 55% of the lymphocytes are prolymphocytes which are large with moderate amounts of pale basophilic cytoplasm, mature condensed chromatin, and a single prominent nucleolus
Chronic leukemias • Hairy cell leukemia • This is mainly a disease of elderly men • Patients present with marked splenomegaly, but not lymphadenopathy • Patients have fatigue and malaise • Pancytopenia • The peripheral smear shows atypical mononuclear lymphocytoid cells with hairy projections on their surfaces • The bone marrow yields a dry tap because the malignant cells are often surrounded by fibrosis • Splenectomy and interferon as well as new chemotherapeutic drugs are successful in promoting long lasting remissions
Chronic leukemias • Large, granular lymphocyte leukemia • T cell or NK cell in origin • Is characterized by a moderate lymphocytosis composed of cells with abundant pale-staining cytoplasm and nuclei with mature, clumped chromatin • Anemia is common, but neutropenia is rare • Most patients survive > 10 years • Sezary’s syndrome • Occurs in patients with cutaneous T cell lymphoma • The lymphocytes seen in the peripheral smear have a very large, convoluted nuclear outline and finely distributed chromatin
Chronic leukemias • Circulating lymphoma cells • Patients with non-Hodgkins lymphoma may develop peripheral blood involvement