Download
1 / 16
160 likes | 279 Views
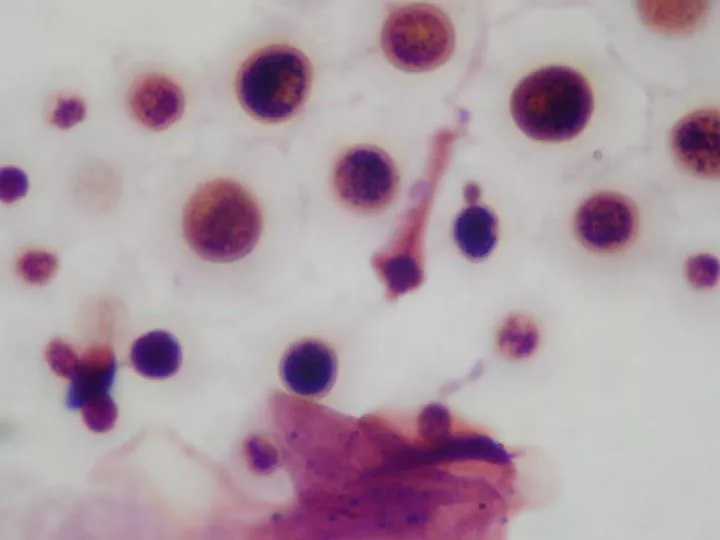
Cryptococcal Meningoencephalitis Nicole Wilde MD, MPH. Nicole Wilde MD, MPH 7/10/09. Cryptococcal Meningoencephalitis. Most typical manifestation Underlying brain parenchyma involved Important OI in immunosuppressed pts. Pathogenesis. C. neoformans inhalation Disseminates hematogenously

E N D
Cryptococcal MeningoencephalitisNicole Wilde MD, MPH Nicole Wilde MD, MPH 7/10/09
Cryptococcal Meningoencephalitis • Most typical manifestation • Underlying brain parenchyma involved • Important OI in immunosuppressed pts
Pathogenesis • C. neoformans inhalation • Disseminates hematogenously • Localizes in CNS • CSF may be good growth medium • Production of mannitol may cause edema and inhibit phagocyte function • Dopamine may promote virulence by serving as a substrate for melanin production
Epidemiology • Majority are immunocompromised • 157 cases, 30% had no apparent underlying condition • HIV, steroid tx, organ transplant, cancer, sarcoid, liver failure
Presentation • Symptoms for several months • Fever in only 50% • HA, lethargy, coma, MS changes, fever • Develop over 2-4 weeks
Cryptococcus in normal host • From 1956-1962: 40 patients age 12 to 66 • 50% with comorbidities • + CSF: 97% • + UCx: 37% • + BCx: 25% • 20/35 had + india ink NEJM 1964; 270: 59
Cryptococcus in normal host • 1957-1969: 31 patients: age 22 to 71 • Sx: HA, fever, wt loss, mental aberration • Signs: fever, AMS, meningeal signs • + CSF cx: 30/31 • 19/27 with + india ink Annals 1969; 71: 1079
Diagnosis • Difficult due to subacute onset • LP necessary • Opening pressure >200mmH2O • India ink 50-75% • Cryptococcal ag testing • Low WBC’s, low glucose, elevated protein • Culture from CSF 3-5 days
Treatment • Uniformly fatal if untreated • Induction, consolidation and maintenance • Amphotericin B 0.7mg/kd/d, Flucytosine 100mg/kg per day, 2 weeks • Fluconazole 400mg day for 8 weeks • Fluconazole 200mg day 1-12 months • Increased intracranial pressure • Lp’s and lumbar shunt
Cryptococcal Meningitis treatment in normal host • 1956-62: 40 patients • 36/40 Rx with AmphoB (? dose) • 31 improved, 5 died • 17/31 relapse free • 11 relapsed, 3 died • Disseminated crypto died • ↑ relapse rate with protein < 100 or cells < 70 NEJM 1964; 270: 59
Cryptococcal treatment in normal host • 66 patients randomized to either 10 weeks AmphoB (0.4mg/kg/d) or6 weeks AmphoB (0.3) + flucytosine (37.5m/k) • 51 adhered to protocol, 27 with ampho alone and 24 with combination • Combo tx w/improvement/cure: 16/24 v. 11/27 • => fewer relapses, quicker CSF sterilization and less nephrotoxicity with combo therapy • Trial stopped early due to clear superiority of combo therapy NEJM 1979; 301: 126
Cryptococcal Meningitis treatment in normal host • 1957-69: 31 patients • All Rx with IV +/- IT AmphoB • 12/31 died Annals 1969; 71: 1079
Prognosis • Underlying illness • Malignancy had shorter median survival when compared to HIV • Relapse vs IRIS • Most are cured
Prognostic factors • 1956-73: 111 patients (most receiving monotherapy) • Death or relapse associated with: • positive india ink • high OP • low glucose • < 20 cells • extraneural + cx • ongoing steroid therapy Annals 1974; 80: 176