Download
1 / 13
130 likes | 302 Views
Anatomy, physiology and pharmacology of the autonomic supply of the heart. The Medulla control centre. The medulla is the primary site in the brain for regulating sympathetic and parasympathetic (vagal) outflow to the heart and blood vessels.

E N D
Anatomy, physiology and pharmacology of the autonomic supply of the heart
The Medulla control centre • The medulla is the primary site in the brain for regulating sympathetic and parasympathetic (vagal) outflow to the heart and blood vessels. • The nucleus tractus solitariusof the medulla receives sensory input from different baroreceptors and chemoreceptors in the circulation. • The medulla also receives information from other brain regions (e.g., hypothalamus). The hypothalamus and higher centres modify the activity of the medullary centres and are particularly important in stimulating cardiovascular responses to emotion and stress (e.g., exercise, thermal stress).
SNS innervation of the heart • Preganglionic neurons of the sympathetic division of the heart originate in the spinal cord and emerge in the spinal nerves at the levels of T-1 through to T-5, then leave the sympathetic chain as post ganglionic neurons travelling to the cardiac plexus.
SNS innervation of the heart • Sympathetic efferents are more diffuse their parasympathetic counterparts, being present throughout the atria (especially in the SA node, but also the AV node) and ventricles, including the conduction system of the heart. Sympathetic nerve endings release Nor-adrenaline.
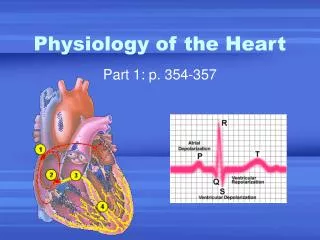
SNS innervation of the heart Obviously, the SNS is stimulated in flight, fight and fright, but cardiac function is also altered by SNS affects on neural activation. When you’re awake: • HR increases (positive chronotropy) • Force of contraction increases (positive inotropy) • AV nodal conduction velocity increases - increased PR interval (positive dromotropy) • Increased rate of myocyte relaxation (positive lusitropy)
PNS innervation of the heart • Supplied by the right (primarily innervates the SA node)and left vagus (left vagus innervates the AV node) nerves (CN X) which provide cervical cardiac nerves to the cardiac plexus. • Unlike the sympathetic innervation, which must first synapse within chain ganglia to supply the heart with postsynaptic (postganglionic) fibres, the parasympathetic fibres synapse at ganglia located directly on the heart and short postsynaptic fibres then supply the target organ. • Atrial muscle is more innervated by vagal efferents than the ventricular myocardium
PNS innervation of the heart ACh released by vagus nerve binds to M2 muscarinic receptors producing: • negative chronotropy • Negative dromotropy • negative inotropy • Negative lusitropy in the atria (the negative inotropic and lusitropic effects of vagal stimulation are relatively weak in the ventricles – since not much PNS representation there).
Messing with autonomic receptors • Β-blockers (especially type 1 selective) will antagonise β-adrenoceptors leading to slower HR, negative inotropy, longer PR intervals etc (eg. Metoprolol, Atenolol, Bisoprolol etc) Used in treatment of Angina, HTN, Heart failure, acute MI, arrhythmias etc. • Muscarinic anticholinergics (eg. Atropine) will antagonise the muscarinic receptors responsible for parasympathetic stimulation of the heart leading to the brakes being removed from the heart, resulting in an increase in HR, shorter PR interval etc used in severe bradycardia and conduction block.
Something quirky The autonomic nerve presynaptic terminals also possess adrenergic and cholinergic receptors that function to regulate the release of Noradrenaline: • Prejunctional α2-adrenoceptors inhibit Noradrenaline release • Prejunctional β2-adrenoceptors facilitate noradrenaline release • Prejunctional M2 receptors inhibit noradrenalin release, which is one mechanism by which vagal stimulation overrides sympathetic stimulation in the heart.