Download
1 / 1
10 likes | 171 Views
ACUTE CARDIAC CARE 2010. Р № 20091. VARIATION OF THE TRANSTHORACIC IMPEDANCE IN A SEQUENCE OF CARDIOVERSION SHOCKS E. Trendafilova 1 , V. Krasteva 2 , TS. Mudrov 2 , JP. Didon 3. 3) Schiller Médical SAS, Wissembourg, France e-mail: jean-philippe.didon@schiller.fr.

E N D
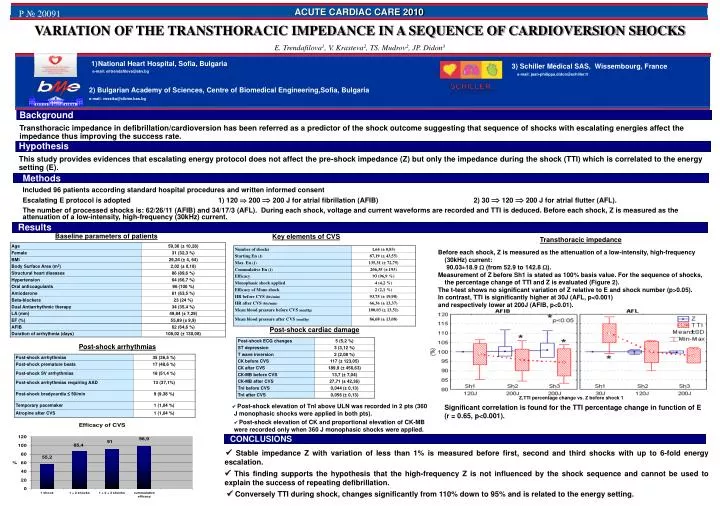
ACUTE CARDIAC CARE 2010 Р № 20091 VARIATION OF THE TRANSTHORACIC IMPEDANCE IN A SEQUENCE OF CARDIOVERSION SHOCKS E. Trendafilova1, V. Krasteva2, TS. Mudrov2, JP. Didon3 3) Schiller Médical SAS, Wissembourg, France e-mail:jean-philippe.didon@schiller.fr • National Heart Hospital, Sofia, Bulgaria • e-mail:elitrendafilova@abv.bg 2) Bulgarian Academy of Sciences, Centre of Biomedical Engineering,Sofia, Bulgaria e-mail:vessika@clbme.bas.bg Background Transthoracic impedance in defibrillation/cardioversion has been referred as a predictor of the shock outcome suggesting that sequence of shocks with escalating energies affect the impedance thus improving the success rate. Hypothesis This study provides evidences that escalating energy protocol does not affect the pre-shock impedance (Z) but only the impedance during the shock (TTI) which is correlated to the energy setting (E). Methods Included 96 patients according standard hospital procedures and written informed consent Escalating E protocol is adopted 1) 120 200 200 J for atrial fibrillation (AFIB)2) 30 120 200 J for atrial flutter (AFL). The number of processed shocks is: 62/26/11 (AFIB) and 34/17/3 (AFL). During each shock, voltage and current waveforms are recorded and TTI is deduced. Before each shock, Z is measured as the attenuation of a low-intensity, high-frequency (30kHz) current. Results Baseline parameters of patients Key elements of CVS Transthoracic impedance Before each shock, Z is measured as the attenuation of a low-intensity, high-frequency (30kHz) current: 90.03±18.9 (from52.9 to142.8 ). Measurement of Z before Sh1 is stated as 100% basis value. For the sequence of shocks, the percentage change of TTI and Z is evaluated (Figure 2). The t-test shows no significant variation of Z relative to E and shock number (p>0.05). In contrast, TTI is significantly higher at 30J (AFL, p<0.001) and respectively lower at 200J (AFIB, p<0.01). Post-shock cardiac damage Post-shock arrhythmias Z,TTI percentage change vs. Z before shock 1 Post-shock elevation of TnI above ULN was recorded in 2 pts (360 J monophasic shocks were applied in both pts). Post-shock elevation of CK and proportional elevation of CK-MB were recorded only when 360 J monophasic shocks were applied. Significant correlation is found for the TTI percentage change in function of E (r = 0.65, p<0.001). CONCLUSIONS Stable impedance Z with variation of less than 1% is measured before first, second and third shocks with up to 6-fold energy escalation. This finding supports the hypothesis that the high-frequency Z is not influenced by the shock sequence and cannot be used to explain the success of repeating defibrillation. Conversely TTI during shock, changes significantly from 110% down to 95% and is related to the energy setting.