Download
1 / 20
200 likes | 279 Views
Reverse Remodeling and the Risk of Ventricular Tachyarrhythmias in MADIT-CRT. Alon Barsheshet , MD 1 , Paul J. Wang, MD 2 , Arthur J. Moss, MD 1 , Scott D. Solomon, MD 3 , Amin Al-Ahmad, MD 2 , Scott McNitt , MS 1 , Elyse Foster, MD 4 ,

E N D
Reverse Remodeling and the Risk of Ventricular Tachyarrhythmias in MADIT-CRT AlonBarsheshet, MD1, Paul J. Wang, MD2, Arthur J. Moss, MD1, Scott D. Solomon, MD3, Amin Al-Ahmad, MD2, Scott McNitt, MS1, Elyse Foster, MD4, David T. Huang, MD1, Helmut U. Klein, MD1, WojciechZareba, MD, PhD1, Michael Eldar, MD5, Ilan Goldenberg, MD1 1Cardiology Division, University of Rochester Medical Center, Rochester, NY; 2Cardiology Division, Stanford University, Stanford, CA; 3Cardiovascular Division, Brigham and Women's Hospital, Harvard Medical School, Boston, MA; 4Department of Medicine, University of California at San Francisco, San Francisco, CA; 5Heart Institute, Sheba Medical Center, Tel Hashomer, Israel
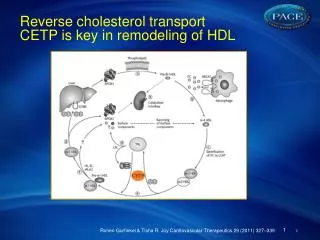
Background • The effect of CRT on the risk of ventricular tachyarrhythmias (VTA) is controversial • Reverse remodeling • LV epicardial pacing • VTA and ICD shocks are associated with reduction in quality of life and with poor prognosis
MADIT CRT • 1820 patients • NYHA class I/II • LVEF <0.30 • QRS > 130 msec • CRT-D or ICD (3:2 ratio) • Mean FU 2.4 years • Clinical outcome • Death or HF event • HR (95% CI) = 0.66 (0.52-0.84) • Echocardiographic outcome
Objective • To explore the association between the magnitude of echocardiographic response to CRT and subsequent risk for VTA in MADIT-CRT
Study Population • 1372 patients • Patients were categorized into 3 groups • CRT-D high echo responders (≥ 25% reduction in LVESV at 1-year) • CRT-D low echo responders • ICD-only patients
Definitions • ΔVolume/ baseline volume = (1 year volume- baseline volume)/ baseline volume • VT: ≤ 250 bpm • VF: > 250 bpm with disorganized EGMs • Vflutter: > 250 bpm and monomorphic
Outcome measures • Primary end point • Appropriate ICD therapy for VTA after the assessment of echocardiographic response • Secondary endpoints • Appropriate ICD therapy for • VTA or death • VT • VF • Vflutter
Statistical analysis • Effect of echocardiographic response to CRT-D on outcome • Categorical variable • Continuous measure • Cox proportional hazards model and a landmark analysis
Clinical characteristics * p<0.05 for comparison among the 3 groups. † p<0.05 for comparison between low and high responders
Echocardiographic characteristics % Volume Change at 1-Year Data are presented as median values
Probability of ventricular tachyarrhythmia by treatment and echocardiographic response
Secondary endpoints p<0.001 p<0.001 p<0.001
Multivariate analysis: Risk of ventricular tachyarrhythmic events Adjusted for age, gender, ischemic etiology, QRS≥150 msec, LBBB, left ventricular end systolic volume indexed to body surface area, and blood urea nitrogen >25 mg/dl.
Multivariate analysis: Secondary endpoints Adjusted for age, gender, ischemic etiology, QRS≥150 msec, LBBB, left ventricular end systolic volume indexed to body surface area, and blood urea nitrogen >25 mg/dl.
Effect of 10% reduction in LVESV among CRT-D patients Adjusted for age, gender, ischemic etiology, QRS≥150 msec, LBBB, left ventricular end systolic volume indexed to body surface area, and blood urea nitrogen >25 mg/dl.
Incidence of VTA by deciles of LVESV change among CRT-D patients
Patients with high echocardiographic response to CRT-D (≥25% reduction in LVESV) exhibit a significant reduction in the risk of VTA events. The magnitude of reverse remodeling is inversely related to VTA risk: 10% reduction in LVESV → 20 % reduction in the risk of VTA. Conclusions
Conclusions • The process of reverse remodeling induced by CRT leads to a lower risk of both HF and arrhythmic events.