Download
1 / 47
800 likes | 6k Views
Cardiac Catheterization Studies. Claire Winters Chief Cardiac Clinical Physiologist TCH. Aims + outcome of lecture. Role of the CCP. Check + use defib, temp pacing + resus equipment Connect up for continuous ECG + sat monitoring

E N D
Cardiac Catheterization Studies Claire Winters Chief Cardiac Clinical Physiologist TCH Claire Winters
Role of the CCP • Check + use defib, temp pacing + resus equipment • Connect up for continuous ECG + sat monitoring • Set up transducer + continually monitor arterial pressure + waveforms • Where applicable record and analyse blood saturations and gases • Log procedure + record required events • Assist with resus • Ensure there own personal safety for radiation • Quality control analysis of blood analysers.
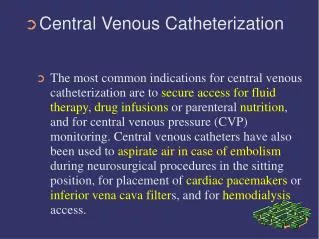
Indications for a left heart catheterisation (LHC) study. • Acute myocardial infarction – with intention of proceeding to PCI • Unstable angina – not controlled by meds. • Chronic stable angina - poorly controlled by meds. • Abnormal EST – positive at low level of exercise (2mm depression, long recovery). • Ventricular arrhythmias – history of SCD without a metabolic cause / sustained vent. arr. • LV dysfunction – assess LV dysfunction / EF • Valvular heart disease – severity of LVOT obstruction, quantify mitral / aortic regurgitation • Preop – ascending aortic aneurysm / dissection • Congenital heart disease • Assessment of artificial valve
Contraindications • Coagulopathy – corrected before cath. Discontinue warfarin 72hrs before procedure. Need INR (international normal ratio) less than 1.8. Heparinized stopped <2hrs before procedure. • Renal failure – increased creatinine - cath deferred. Dialysis pt – cath deferred until after dialysis. • Dye allergy • Infection • Lab abnormalities – anaemia, electrolyte imbalances • Decompensated heart failure best to optimise med therapy before cath. • Severe peripheral vascular disease – claudication – assess pulse • Abnormal aortic aneurysm – special care – use of radial approach • Uncontrolled hypertension – maximise safety at access site.
Pt preparation • Informed consent – benefits, risks • Assessment – history, physical exam, peripheral pulses, labs, blood count. • Meds – if PCI likely pt needs asprin • Fast 4hrs before
Procedure • Set up and monitor ECG, set transducer • Log pt events • Sedation if required - diazepam • Arterial access • Ensure pressure manifold is working properly • Insert catheters • Record cardiac pressures • Inject contrast into the RCA, LCA and LV angio if required. • Remove catheters
Arterial access 1) RFA – easy access, low complications Palpate RFA - once obtained clean site with Betadine and surgically drape Infiltrate 1 -2% lignocaine subcutaneous about 2 – 4 cm below the inguinal ligament using an angle needle 45o to skin – (see diagram) Insert access needle 16 – 18 gauge Cook needle – aim in same direction to puncture artery – access gained by observing a brisk ‘spurt’ of red blood – sluggish backflow venous access. Insert 0.035inch J tipped guidewire to the abdominal ao, needle is then withdrawn. Arterial sheath with dilator, arterial sheath has a haemostatic device and side port is placed over the wire. Wire and dilator is then removed Sheath is then flushed with saline. 6F or 5F sheath generally used. 2) Brachial / radial approach - Artery palpated medially in the antecubital fossa Approach similar to cut down technique for the RFA approach. Left arm approach Judkins catheter is adequate R. arm approach Amplatz or MP catheter
Transducer • Converts mechanical pressure of the blood in the cardiac chamber / vessel to an electrical signal • The transducer must not alter the event being measured • It must be specific • Have amplitude linearity i.e. output amplitude proportional to input amplitude • Adequate frequency response – output ratio : input amp over a range of frequencies • Freedom from distortion – transducer maintains time differences in the wave freq.
Transducer used in cath. lab employs principle of a Wheatstone bridge – i.e. the strain gauge is a variable resistance – when the wire stretches its electrical resistance increases. • Increase pressure stretch in the diaphragm increases electrical resistance as long as strain remains below the elastic limit of the wire. • Transducer in cath lab generally has a silicone diaphragm – acts as a sensor element. A sterile dome is attached to the transducer and tubing to the catheter. Fluid pressure from the blood is transmitted to sensing element through a gel medium thus bending the circuit altering resistance of the resistor. The circuit delivers an electrical output proportional to the pressure being applied – i.e. high amplitude output for arterial pressures and less for venous. • Transducer attached to the table should be as close to the catheter as possible. • Optimal pressure measurements – length of tubing from catheter to transducer should be as short as possible.
Zero reference • Pressure measurement meaningless unless an accurate zero reference is obtained prior to cath. • Location – mid chest diameter i.e. mid anterior-posterior • Tubing is attached to an adjustable pole on the table and a spirit level is used to accurately measure the mid AP • If transducer above mid AP – inaccurate low pressure, below – inaccurate high pressure • Calibration – Tubing and transducer dome are filled with saline from flush line and all bubbles are removed. • Zero port is open to room air output signal is adjusted to read 0. • Pressure generator of 100mmHG is transmitted to the transducer and recorded– pulse generator runs (10cm to 100mmHg)
Manifold • System that is attached to the catheter tubing • Consists of a syringe, connector tubing, series of 3 way taps (valve ports) which connect to the pressure transducer and zero line, a port for saline flush, waste flush port and a contrast agent reservoir. • Dr ensures there is no air in catheter and tubing by aspirating air in the catheter before starting and injections
Other equipment • Image intensifier (fluroscope) mounted on a C arm • Injector pump – rate controlled bolus • Physiological monitor / recorder • Pressure amplifier
LV angiogram • Used to assess LV function, MR, VSD • Pigtail catheter advanced to the descending aorta, aortic arch to the aortic root. • Aortic pressure recorded at this level • Catheter advanced past the aortic valve to the LV – pressure sampled – ectopics may be observed during catheter placement. • Ideally catheter advanced to the LV apex to avoid catheter induced MR • LV angio performed while pt hold his breath. Pt advised about hot flushing sensation • LV pressure sampled post angio. • Pull back – record pressure gradient between the LV and AO as the catheter is advanced back from the LV through the aortic valve to the aorta. • Contraindications:- Critical aortic stenosis, significant LMS or severe LV dysfunction.
Aortogram • (If needed) required for aortic insufficiency, diseases of the aorta – aneurysms, dissections, non selective shots for anomalous coronary arteries or grafts that are difficult to engage. • Use same catheter as used for LV angio. • Catheter positioned 3-7cm above the aortic valve. • Renal angiogram - can be done when catheters are being removed at the end of the procedure to assess the renal arteries.
ECG changes • LMS – pressure dampening • LCA – Anterior changes – T wave inversion • Cx – T wave inversion lateral • RCA – inferior changes, heart block – hit against SA nodal branch • LV angio – lodging catheter in the LV - VEs • Damping – catheter wedges into and occludes an artery pressure trace may ‘ventricularize’ (low diastolic pressure) – watch far hypotension, arrhythmias – remove catheter
Graft study • Review of surgery notes to determine which grafts are attached to what veins • Aortogram required • Internal mammary artery left, right (LIMA, RIMA) • Saphenous vein grafts (SVGs) • Observe graft markers
Post catheter care • Sheath removal –Catheters + sheath removed at the end of the procedure. • Bed rest for 6hrs, 2hrs for arm • Observation required hr, bp, temp, distal pulses + entry site. • Some pts may require fluids
Closure devices • Hemostasis – manual pressure • Femstop • Angioseal - puncture closure device –biodegradable collagen plus deployed to FA – foreign material, arterial site can’t be used for 45-60 days after. • Perclose – percutaneous vascular suture device
Complications • Death • MI • Stroke – air embolus / thrombus • Coronary artery dissection • Coronary artery spasm • Renal failure • Emergency bypass • Arrhythmias • Vagal reaction • Vascular – sheath removal • Bleeding – access site • Infection • Allergy
Percutaneous coronary intervention (P.C.I) Interventional cardiology • Procedure similar to that of an angio • Measure up area of blocked artery • Antiplatelet therapy pretest • ACT • Heparainsie • Catheter • Guidewire • Direct stent • Predilate with angiographic balloon (central lumen is flushed with heparinized saline, emptied and replaced with contrast) this is then placed over the guidewire. Balloon has markers to guide its position, screen, incorrect position balloon is gently inflated. Several inflations can be made then deploy a stent • Postdilate
Equipment • Guidewires - Stiffness – floppy, intermediate, standard • Strength – extra support • Coating – hydorphilic • Calibre – usually 0.014in • Balloons – length, diameter • Compliant – inflation pressure increases so does the balloon diameter – ‘nominal’ pressure • Non compliant expand little beyond stated pressure – used for calcified lesions or overlap between stents • Stents • Bare metal – flexible, laser cut polished, balloon mounted, expandable stainless steel • Drug eluting – antiproliferation agents such as rapamycin or piclitaxel – prevent miototic growth (inflammation)
Other equipment used for interventional cardiology • Intravascular ultrasound (IVUS) up to 40MHz -Allows a cross-sectional image of the lumen and vessel wall – greater accuracy in measurement due to better spatial resolution. • Allows proper assessment of stent deployment, clarify anatomy • Pressure wire for fractional flow reserve (FFR) • Used when a lesion is present and operator is determining if it should be treated medically or with intervention. • Wire allows direct measurement of intracoronary pressure • Wire with a pressure transducer placed initially in coronary ostium and calibrated then moves distally beyond the stenosed artery and the translesional gradient is measured. • Allows calculation of the FFR – ratio of distal coronary pressure to aortic pressure through hyperemia. • Vasodilator – adenosine infusion is used • FFR 1 – normal no intervention required, FFR <0.75 intervention required
cont • Cutting balloon atherectomy - Has 3 – 4 razor atherotomes which cut into plaque and vessel wall and allow vessel dilation at a low balloon pressure. • Rotoblator • Uses 160,000 rpm diamond-coated burr (drill) advanced over a 0.009inch wire to the coronary lesion to break away calcified plaques • Sluggish flow can occur therefore vasodilators are required • High risk procedure, temporary pacing required for backup • Filters • Collapsible filters mounted on the distal end of a 0.014 wire advanced downstream of the lesion. • When deployed porous devices appear like an umbrella and allow blood to flow through while filtering any debris (plaque) is retrieved
Right Heart Cath Claire Winters
Indications • Acute MI – complications by hypotension, congestive heart failure, sinus tachy, RV infarct, or mechanical complication VSD, pericardial tamponade or acute regurgitation. • Assess volume status whom physical signs may be unreliable • Severe LV failure – guide in inotropic, diuretic and afterload management • Cardiac tamponade – PA cath • Cardiogenic shock • Biopsy of right sided structures • Differentiate between pericardial and constrictive pericarditis • Severe pulmonary hypertension – PA pressure • High risk cardiac patients pre, intra and post-op pts • Paediatrics – shunts –VSD, ASD, hypoplasia, univentricular heart, Fallots, transposition,
Contraindications • No absolute but relative include profound coagulopathy (inr >2) • LBBB relative contraindication since one of the risks of a PA catheter is RBB.
Catheter • Access: - Internal jugular vein, subclavian vein, femoral vein • Catheter Swan-Ganz or PA flotation catheter. Single lumen opens catheter tip and allows pressure measurement of the PA and pulmonary capillary wedge pressure (PCWP). Inflation of to balloon in a branch of the PA occludes antegrade PA flow – pressure at tip represents LA pressure
Method • Flush all catheter lumina • Test floatation balloon before introducing into vein • Zero pressure transducer (at RA) • Pass catheter down venous sheath, guide into ra • Inflate balloon to float catheter into RA and RV • Advance catheter with balloon inflated until PA pressure trace damps or catheter tip lodges into the branch PA • Record pressure readings and oxygen saturations from RA, RV, PA and wedge • Accurate recording of PCW pressure – balloon inflated and clear PA tracing with the balloon deflated.
RA – Systole occurs after P wave on ECG. - X - Atrial relaxation with decline in pressure. Tricuspid closure –upright deflection i.e. c wave – follows PR interval V wave – near end of T wave – atrial filling Y wave descent – opening of tricuspid valve with emptying of the atrium. Normally a wave is greater than peak v RV - peak systolic and end diastolic wave are used for RV pressure PA – peak systolic, end diastolic and mean pressure are measured PCWP – i.e. LA pressure – wave similar to the RA pressure V wave is greater than the a wave Mean PCW, a wave and v wave are recorded Pressure wave forms
Changes in pressure wave forms • RV failure: - RV infarct, severe pulmonary hypertension, pulmonary embolism – causes increased RAP and RVEDP, low CO and BP. Because RV dilates a dip on the plateau is seen, RA – steep y descent • Acute MR:- LA subjected to increased pressure. Regurg. produces a large v wave after the T wave. V wave x 2 value of PWCP abnormal – suggestive of severe MR. Other causes of large V wave – TR, VSD. • AR – low AO diastolic pressure, LV workload increases, thus increasing diastolic volume of the LV leading to more forceful contractions – increase EDP • MS – Simultaneous record LV and PW pressure – mean LV diastolic pressure remains the same, LA mean increased progressively • Acute TR – RA systolic wave may resemble the RV trace. There is increased RA and RV EDP – prominent V wave observed. • Cardiac Tamponade – equalization of RAP, RV and PCW and increased mean pressure • Pulmonary embolism – Ventricularization of the PA wave form with a rapid end diastolic descent and barely visible dicrotic notch
Oxygen saturations • Definition: ‘the amount of oxygen carried by haemoglobin (oxygen content) compared to the amount that could be carried (oxygen capacity)’
Cardiac Output (CO) calculation using Fick Principle • CO –quantity of blood ejected from the heart/min i.e. Stroke vol (ejection/ beat) x hr • Simplest method of calculating CO based on the amount of O2 absorbed during normal ventilation by the lungs i.e. arterial minus venous O2 sat – need 2 blood samples AO and PA • Amount O2 removed is divided into the O2 consumption i.e. amount of O2 consumed by the body in mls/min (O2 consumption taken from table based on pts age, sex and BSA). • FORMULA for CO :- Oxygen consumption ÷ 10 l /min Art – ven O2 sat Vols %
examples of COP calculations Claire Winters
cont • O2 sat is expressed as O2 content (Vols% not %sat) O2 sat is the % haemoglobin which is oxyhaemoglobin i.e. the amount of O2 carried by the haemoglobin – the O2 content compared to the amount that could be carried – the O2 capacity • Therefore need to convert O2 sat into Vols% for Fick calc. • 1gm Hb has the capacity to combine with 1.34cc oxygen. If Hb is 13.0gm/dl max capacity for O2 is 13.0 x 1.34 = 17.2vols
cont • e.g. AO sat 96%, PA sat 72%, Hb 13.5gm/dl and assume O2 consumption is 180mls/min. What is the CO? The O2 capacity = 13.5x1.34=18.09 vols% (for O2 sat) PA sat in vols%=72x18.09 ÷100 = 13.03 AO 96x18.09 ÷100 = 17.30 CO is Oxygen consumption ÷ 10 l /min Art – ven O2 sat Vols % 180 ÷10 vols% 180 ÷ 10 = 4.14 l/min 17.36-13.02 4.34 Normal cardiac output - 4 – 8 L
cont • Cardiac Index CO/BSA Normal 2.8 – 4.2L/min/m2 • Stroke vol CO/heart rate • Pulmonary vascular resistance = (mean PAP–PCWP) x 80 N=100-250 dyne.s cm CO • Systemic vascular resistance (mean SAP-mean RAP)/CO x 80 N=770 – 1500 dynes.s.cm
Shunt calculation • Ratio of pulmonary to arterial flow i.e. Qp:Qs (arterial saturation – mixed venous saturation) (pulmonary vein sat – pulmonary artery sat) Mixed venous – 3 x SVC + 1 x IVC 4 e.g. IVC 78%, SVC 74%, RA 76%, PA 89%, LV 96%, AO 96% what is the shunt? SA 96 – (3x74 + 78 / 4) 75 = 21 PV 96 – PA 89 = 7 Shunt =3 Ratio greater than 2 generally means pt would benefit from surgery.
e.gs. of shunt calcs Claire Winters
Thermodilution method for CO • Swann Gantz catheter with a thermister at its tip and a lumen prox. to this is situated in the PA. Bowl of dextrose is set up in a bed of ice with a thermometer. • Catheter is connected to a single purpose electronic computer and a pen recorder. • Baseline on recorder and computer are stabilised and calibration signal is given – provides reference - no of mm deflection a 1 degree C temp change will produce. On computer body temp and catheter constants are set. • Each injection 10mls of ice cold dextrose is drawn up into a syringe and temp is noted. • Contents of the syringe are quickly injected via the first lumen – usually the RA. The chilled solution becomes mixed with blood by the time it reaches the PA – this mixture is cooler than blood alone and the temp change is sensed by the thermister and changes electrical resistance. • The change recorded is proportional to the volume of cold dextrose injected and volume which has been added. The change is displayed as a curve and a digital display of the CO is obtained.