Download

1 / 27
280 likes | 467 Views
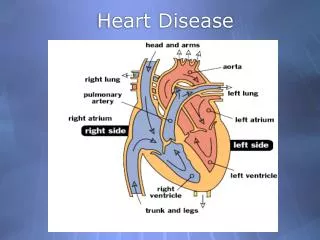
Pediatric Heart Disease. Infants may have one of the following: Cyanosis (cyanotic CHD or R to L shunt) Pulmonary and tricuspid atresia CHF (L to R shunt) or shock Shock from outflow obstruction Diagnostic evaluation CXR EKG. Cyanotic Heart Defects. T etralogy of Fallot

E N D
Infants may have one of the following: • Cyanosis (cyanotic CHD or R to L shunt) • Pulmonary and tricuspid atresia • CHF (L to R shunt) or shock • Shock from outflow obstruction • Diagnostic evaluation • CXR • EKG
Cyanotic Heart Defects • Tetralogy of Fallot • Transposition of the great vessels • Truncus arteriosus • Total anomalous pulmonary venous return • Tricuspid valve Abnormalities • Severe pulmonic stenosis
Tetralogy of Fallot • Consists of VSD, obstructed right vent. outflow tract, dextroposed overriding aorta, RVH. • TeT spells-worsening obstruction of flow in the pulmonary artery leading to greater R to L shunt. Causes cyanosis and dyspnea.
Transposition of Great Vessels • Appears in 1st week of life. • Aorta comes from R vent. and pulmonary art. Comes from L vent. • Must have a VSD or ASD for survival • If suspected, start Prostaglandin E1
Truncus Arteriosus • Large arterial trunk from the ventricular portion of the heart. • Supplies blood to systemic and pulmonary circulation. • Present with increased pulm. blood flow, dyspnea and CHF
Coarctation of the Aorta • Narrowing of the aortic lumen. • Present with CHF and feeding difficulty. • Decreased pulse amplitude in the lower ext. • Hypertension in the upper ext. • Older kids present with exercise intolerance and rib notching.
Ductal Dependent heart defects • Depend on a patent ductus arteriosus. • Systemic blood flow depends on a R to L shunt from the pulmonary artery through the DA to aorta. • Pulmonic blood flow depends on a L to R shunt from the aorta through the DA to the pulmonary art.
Defects dependent on R to L shunt via the PDA include: • Critical Aortic Stenosis • Hypoplastic left heart • Severe coarctation • Usual Clinical Presentation • Circulatory collapse at the end of first week of life
Treatment • Prostaglandin infusion keeps the DA open until surgery. • Start at 0.1 mcg/kg/min and titrate
CHF • Usually w/in the first 6 months when PVR has decreased allowing L to R shunt (VSD or PDA) • Triad of CHF in infancy • Tachypnea • Tachycardia • Hepatosplenomegaly
Treatment • Supportive • Lasik • Digoxin except in IHSS or TOF • Inotropes • Pressors • Vasodilators • Afterload reducing drugs • Head up • NPO • Treat infections
Atrial septal defects • RA and RV enlargement • Pulmonary over-circulation • High pressure • Low volume • ASD low morbidity and mortality • Repair may be surgical or trans cath
Most common CHD May occur in any septal location Hemodynamic significance depends on the size of the defect. Spontaneous closure in the first 6 mo. In 30-40%. Surgical repair required if: Infant has failure to thrive Pulmonary HTN R to L shunt Vent. Septal Defect
Aortic Stenosis • May have a mono, bi or tricuspid valve. • If severe, avoid prosthetic valve until they are old enough to receive an adult sized one.
In critical AS, LV unable to pump adequate flow past the aortic valve. • If no PDA, not compatible with life
Kawasaki’s Disease • Acute self limited multisystem vasculitis • Clinical presentation • Fever 5 or more days with 4 of 5 other clinical features • Bilat. conjunctival inection w/o exudates • Mucous membranes changes of upper resp. tract Erythema and edema of hands/feet (early) and desquamation (subacute phase) • Exantham polymorphous, truncal • Acute cervical lymphadenopathy
Lab findings include high WBC, left shift, hemolytic anemia, high platelets, high CRP/ESR, pyuria, bilirubinuria • On CXR infiltrates, cardiomegaly, long PR or QT, dysrhythmias • Cardiac echocardiography show coronary aneurysms 80-90% of time
Treatment • Hospitalization for IVIG • ASA • Cardiac eval. • Corticosteroids may decrease coronary aneurysms
Myocarditis • Causes • Idiopathic • Inflammatory • Acute rheumatic fever • Collagen vascular disease • Lyme disease • Toxins • HIV • Viruses • Adenovirus • Coxsackie A and B
Often misdiagnosed • Classic presentation • CHF or fulminant cardiogenic shock • Syncope from dysrhythmias May present with cough, wheeze/tachypnea, congestion, or fever. Consider in a child with wheezing and no history of asthma or in a febrile child whose wheezing is not responding to treatment.
Diagnostic eval • CXR-cardiomegaly • EKG changes • Elevated troponin • Definitive diagnosis-biopsy or MRI
Treatment • Bedrest • Oxygen • Inotropes • May need transplant 35% mortality
SVT • Most common dysrhythmia • Present with tachycardia, poor feeding, tachypnea, pallor, lethargy, chest pain. • HR usually >230 BPM • Unstable sync. Cardiovert 0.5 j/kg. Lidocaine 1 mg/kg should be given prior d/t risk of V fib. • Adenosine 0.1 mg/kg the 0.3 mg/kg
A fib Usually d/t rheumatic heart disease or dilated cardiomyopathy. Unstable-cardiovert 0.5 J/kg Medical therapy (dig) is usually not effective Anticoagulation is not necessary
V Tach • Usually seen with congenital heart disease, but also with myocarditis, cardiomyopathy, or prolonged QT. • Unstable sync. Cardiovert 1-2 J/kg • Start Lidocaine or Procainamide if pt not stable for transfer
V Fib • Initial energy for defib is 2 J/kg. Can be doubled. • A trial of amiodarone 5mg/kg infusion followed by defib. • If successful, Amiodarone infusion 5-15 micrograms/kg/min. • After 3 defib attempts and a second 2 mg/kg bolus infusion usually indicates futility.