Download
1 / 18
190 likes | 376 Views
Schistosomiasis. By Mohammed Mahmoud, MD Lecturer of tropical Medicine Cairo university. Specices & Distribution. S. Mansoni : Nile valley, Sudan, Brazil and Venzezuella S. Haematobium : Upper Egypt, Africa, Western Asia S. Japonicum: Far East. Life Cycle. Basic pathology.

E N D
Schistosomiasis By Mohammed Mahmoud, MD Lecturer of tropical Medicine Cairo university
Specices & Distribution • S. Mansoni : Nile valley, Sudan, Brazil and Venzezuella • S. Haematobium: Upper Egypt, Africa, Western Asia • S. Japonicum: Far East
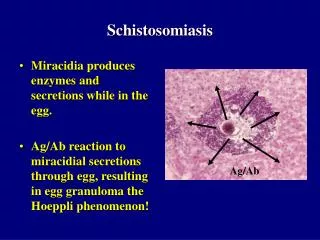
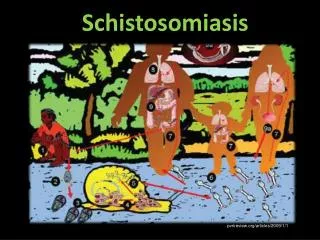
Basic pathology • Cercaria Allergic dermatitis • Adults No harm • Eggs granulomas Fibrosis egg antigens immune complexes Katayama fever
Clinical picture • Cercarial dermatitis: pruritic rash occurs within 24 h of cercarial penetration • Katayama fever: - Usually with S. japonicum (???) - Heavy infection with mansoni - Occur in non-immune persons - 4-6 weeks after primary infection (time of egg deposition) - Fever, rigors, HSM, LN, ulticarial rash, marked eosionophilia
Urogenital schistosomiasis: - S.haematobium - affect UB, ureter, genital organs - Dysuria, terminal haematuria Complications: 1- Obstructive uropathy 2- Cancer bladder (squamous cell)
Intestinal schistosomiasis: - caused by mansoni - affect large bowel (rectum and sigmoid) - due to submucosal egg deposition granumona fibrosis- Clinically: 1- Bilharzial dysentery dysentery, tensmus, mucus in stools, crampy abdominal pain 2- Colonic polyposis Bloody diarrhea, anemia, hypoprotinemia, clubbing of fingers (never turn malig) 3- Bilharzioma: Tender palpable mass in Lt iliac fossa Never turn malignant
Hepatic schisosomiasis • Caused by S. Mansoni, S. Japonicum • Stages: 1- Stage of hepatomegly: ovideposition and granuloma formation liver is enlarged, smooth, firm, rounded edge. 2- Stage of HSM (Mainly due RES) 3- Stage of Huge splenomegly (PH) and shrunken liver (periportal fibrosis) and PS collaterals. 4- Stage of ascites (PH and hypoprotinemia, late due to malnutrition, loss of proteins by colonic polyposis and haematemesis) 5- Terminal hepatic failure concomitant viral hepatitis Reversal of the blood flow away from the liver (PS)
Cardiopulmonary Schistosomiasis • Larval Pneumonitis: allery to schistosomulae migrations low grade fever, cough, haemoptysis, wheezes, eosionophilia • Core pulmonale: due to eggs of S. mansoni (reach through PS collaterals), S. haemtobium pulmonary arterioles granuloma fibrosis endertaritis oblitrans pulmonary HT RVH RVF X-ray dilatation of main pulmonary arteries (Dumble shape masses at the hilum)
Ectopic Schistosomiasis • Due to aberrant migration of the eggs • Mainly affect brain (seizures), spinal cord (paraplegia), eye (visual field defects), skin.
Chronic salmonellosis • Salmonella behave atypical in cases of schistosomiasis following a rather chronic course unlike the usual acute illness • Due to proliferation of salmonella in the gut of the adult schistosomes, shedding salmonella into blood chronic bacteraemia prolonged fever • Ttt by antityphoid to eradicate salmonella and prevent relapse by antischistosomal therapy.
Diagnosis • Stool and urine examination • Rectal snip (gold standard) • Liver biopsy • Serological tests: • Ab detection donot differentiate between active and past infection, did not decrease after ttt • Ag detection indicate active infection and decrease after successful ttt
Treatment • Praziquantel (Drug of choice) for both mansoni and haematobium, 40 mg/kg, can be repreated 2 or 3 times in moderate and severe infections • Metrifonate: for S.haematobium 10 mg/kg in 3 repeated doses at 2 weeks interval • Oxamniquine: for mansoni 20 mg/kg daily for 3 days