Download
1 / 16
160 likes | 330 Views
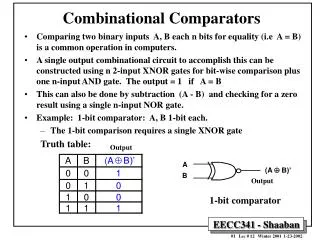
Low Intensity Comparators for Interpersonal Psychotherapy Trials. Holly A. Swartz, M.D. Yu Cheng, Ph.D. University of Pittsburgh School of Medicine Pittsburgh, PA USA. Disclosure. Examples of Low Intensity Comparators. No active treatment Wait list control (WLC)

E N D
Low Intensity Comparators for Interpersonal Psychotherapy Trials Holly A. Swartz, M.D. Yu Cheng, Ph.D. University of Pittsburgh School of Medicine Pittsburgh, PA USA
Examples of Low Intensity Comparators • No active treatment • Wait list control (WLC) • Non-scheduled treatment control • Non-standardized treatment • Treatment as usual (TAU) • Usual care (UC)
Characteristics of No Active Treatment Controls • Minimum/low contact condition • Assessments only • Subjects withdrawn for clinical worsening and offered active treatment • Expectation of eventual care (if study offers intervention at the end of trial to those who did not receive it)
Characteristic of TAU/UC • Subjects are free to seek care in the community • Nature of treatment received is usually quite variable • Some studies augment the referral process • Treatment is provided outside of the research protocol
Advantages of Low Intensity Comparators: TAU/UC • Answers important questions: • “How does IPT compare to services as they are provided in usual care settings?” • “Does IPT offer incremental advantages over current practice?” • Ecological validity • Patients are afforded a range of treatment options • Bottom line • Increased external validity (generalizability) of trial • Low(er) costs for clinical trial
Disadvantages of Low Intensity Comparators: TAU/UC • TAU/UC is very variable • Difficult to know what patients are actually getting • Unmeasured in most trials • Decreased comparability across trials* • Does not control for nonspecific factors associated with a clinical trial • Fewer resources(financial/personnel) in community • Differential incentives for treatment engagement • Lacks Hawthorne effect of addition of study intervention • Bottom line • Decreased internal validity of trial *Poses additional dilemmas when comparing studies across countries where standards of community care differ
Advantages of Low Intensity Comparators: WLC • If sample is non-treatment seeking, may be proxy for “usual care” • Controls for the natural course of untreated illness (i.e., scientific interest) • Low(er) costs for clinical trial • Bottom Line • Few advantages
Disadvantages of Low Intensity Comparators: WLC • Ethical concerns • Withholding treatment from a vulnerable population • High dropout rates (in some trials) • Does not control for non-specific factors of IPT • Support • Contact hours • Helping relationship • Even if IPT “wins,” you’ve shown that it is better than no treatment, which is not much of a victory • Bottom line • Decreased internal validity • Hard to justify WLC
IPT v. WLC or Non-Scheduled Treatment: ES 1ES calculated comparing IPT to WLC using reported values, Morris S. Estimating effect sizes from pretest-posttest-control group designs. Organizational Research Methods (2008); 11:364-386. 2SD deviations not reported, therefore assumed SD=SD of other studies reporting depression scores as HRSD-17
IPT v. WLC or Non-Scheduled Treatment: NNT 1NNT calculated from reported categorical response/remission rates rather than ES, as per Furukawa TA, Leucht S (2011) How to Obtain NNT from Cohen’s d: Comparison of Two Methods. PLoS ONE 6(4): 19070.doi:10.1371/journal.pone.0019070
IPT v. TAU or UC: Effect Sizes 1ES calculated comparing IPT to WLC using reported values, Morris S. Estimating effect sizes from pretest-posttest-control group designs. Organizational Research Methods (2008); 11:364-386. 2ES reported in the original manuscript
IPT v. TAU or UC: Effect Sizes, cont. 1ES calculated comparing IPT to WLC using reported values, Morris S. Estimating effect sizes from pretest-posttest-control group designs. Organizational Research Methods (2008); 11:364-386.
IPT v. TAU or UC: NNT 1NNT calculated from reported categorical response/remission rates rather than ES, as per Furukawa TA, Leucht S (2011) How to Obtain NNT from Cohen’s d: Comparison of Two Methods. PLoS ONE 6(4): 19070.doi:10.1371/journal.pone.0019070
IPT v. TAU or UC: NNT, cont. 1NNT calculated from reported categorical response/remission rates rather than ES, as per Furukawa TA, Leucht S (2011) How to Obtain NNT from Cohen’s d: Comparison of Two Methods. PLoS ONE 6(4): 19070.doi:10.1371/journal.pone.0019070
Summary • Some low intensity comparators (TAU/UC) have advantage of comparing IPT to “real world” conditions • Many disadvantages to this model (ethical concerns, lack of control for nonspecific factors of both clinical trial itself and psychotherapy, variability and lack of measurement of intervention) • Yields large effect sizes