Download
1 / 41
421 likes | 633 Views
OMT of the Thoracic Spine. Eric J. Milie D.O. Internal Medicine Lecture Series 1/5/04. Objectives:. The physician will become comfortable with the osteopathic manipulative treatments demonstrated during the lecture

E N D
OMT of the Thoracic Spine Eric J. Milie D.O. Internal Medicine Lecture Series 1/5/04
Objectives: • The physician will become comfortable with the osteopathic manipulative treatments demonstrated during the lecture • The osteopathic physician will be able to name thoracic spine and rib dysfunction • The osteopathic physician will understand the complex anatomy of the thoracic spine and thoracic inlet/outlet
Evidence Based Medicine • DR Noll, et al. Benefits of osteopathic manipulative treatment for hospitalized elderly patients with pneumonia. JAOA • Vol 100 • No 12 • December 2000 • 776-782 • Showed that hospitalized pt’s treated with OMT required significantly shorter courses of intravenous antibiotics and also had a significantly shorter hospital stay • Andersson GB, Lucente T, Davis AM, Kappler RE, Lipton JA, Leurgans S. A comparison of osteopathic spinal manipulation with standard care for patients with low back pain. N Engl J Med.1999; 341:1426 –1431 • Patients treated with OMT required less analgesics than patients treated with “standard medical therapy” alone, and were more satisfied with their care
Evidence Based Medicine cont. • Hoehler FK, Tobis JS, Buerger AA. Spinal manipulation for low back pain. JAMA.1981; 245:1835 –1838 • Showed that patients treated with OMT received equal benefit compared to patients receiving analgesics and soft tissue massage • Licciardone JC, Stoll ST, Fulda KG, Russo DP, Siu J, WinnW, et al. Osteopathic manipulative treatment for chronic low back pain: a randomized controlled trial. Spine.2003; 28:1355 –1362 • Patients with chronic back pain who received osteopathic manipulation reported greater improvements in back pain, greater satisfaction with back care throughout the trial, better physical functioning and mental health at 1 month, and fewer cotreatments at 6 months compared to the control group
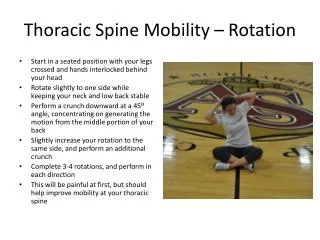
Thoracic Motion • Upper and middle thoracic: Rotation> flexion/extension> sidebending • Lower Thoracic: Flexion/ extension> sidebending> rotation • Main motion of T-spine: Rotation
Anatomical Landmarks • Spine of scapula- T3 • Inferior angle of scapula- T7 • Sternal notch- T2 • Sternal angle (angle of Louis)- T4, attaches to 2nd rib • Nipple- T4 Dermatome • Umbilicus- T10 dermatome
The motion of the 1st and 7th ribs in A, ordinary expiration; B, quiet inspiration, and C, forced expiration
Rib Motion with Respiration • Bucket-Handle Motion -- Characteristic rib motion, primarily of the lower ribs, that occurs during respiration. The effect is to increase the transverse diameter of the thorax during inspiration. This involves ribs 7-10 • Pump-Handle Rib Motion -- Characteristic rib motion, primarily of the upper ribs, that occurs during respiration. The effect is to increase the anteroposterior diameter of the thorax during inspiration. This primarily effects ribs 1-6. • Caliper motion: Ribs 11, 12
Exhalation vs Inhalation Ribs • Exhilation Rib: A somatic dysfunction usually characterized by a rib being held in a position of exhalation such that motion toward exhalation is more free and motion toward inhalation is restricted. Also called “inhalation restriction.” • Inhalation Rib: somatic dysfunction usually characterized by a rib being held in a position of inhalation such that motion toward inhalation is more free and motion toward exhalation is restricted. Also called “exhalation restriction.” • In exhalation dysfunction, the “key rib” is uppermost rib of dysfunction, in inhalation dysfunction, it is the lowermost rib
Rib Raising • Reduces constriction of large lymphatic vessels • Stimulates regional sympathetic efferent activity • Results in prolonged reduction in sympathetic outflow • Excursion of chest is increased and lymphatic flow is improved
Rib Raising cont. • Patient Position: Supine • Physician Position: Standing or seated at the patient’s side
Rib Raising Procedure • Palms placed under patient’s thorax, so that pads of fingers at rib angles • Flex fingers, apply traction to the rib angle • While applying traction, bend knees/ lower trunk to raise ribs (lever/fulcrum action) Do not bend wrists • Move hands so that subsequent ribs treated • Treat opposite side of rib cage in same manner
Respiratory Diaphragm Release Technique • Dysfunction: Tension and reduced excursion of the respiratory diaphragm and the lower thoracic cage • Objective: To three-dimensionally balance thethoracic spine, and the costo-diaphragmatic relationships • Physician Position: At the head of the patient or the side of the patient • Patient Position: Lying supine
Respiratory Diaphragm Release Procedure • Patient seated or supine • Physician standing behind patient or at patient’s side • Physician’s hands around thoracic cage, fingers under the costal margin • Check motion by gently rotating thoracic tissues • Treatment Phase: Hold thoracic tissues in the direction in which they move freely. Allow fascia to unwind, until it settles into a rhythmic vertical motion
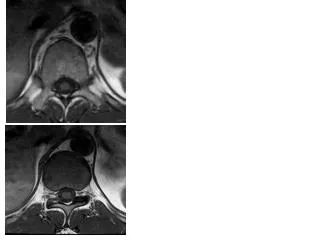
Thoracic Outlet • Roughly 4cm area boundaried anteriorly by the manubrium of the sternum, laterally by the 1st rib and its costal cartilage, and posteriorly by the body of T1 • Covered by Sibson’s fascia, surrounded by the scalenes, SCM, and the trapezium • Subclavian vein and artery, brachial plexus, and lymphatics run through these structures
Thoracic Outlet Release • Purpose: To relax soft tissue restrictions and enhance lymphatic drainage from the head and neck • Physician Position: Sitting at head of table or side of patient • Patient Position: Lying supine
Thoracic Outlet Release technique • Place one hand posterior to the thoracic inlet (transversely) at the level of the first and second ribs. • Place the other hand at the same level on the anterior chest wall. • The area is motion tested for myofascial restrictions. These motions include a side-to-side movement, a rotational or twisting movement, a superior or inferior movement, or an angular movement. • The area is treated directly (barrier engagement) or indirectly (position of fascial ease). Having the patient take three deep breaths, can facilitate a release. • The physician waits for a release and the area is re-evaluated. • Modification: Both hands can also be placed on the anterior thorax. With this position, the thumbs contact the trapezius muscle and posterior upper two ribs. The fingers lie on the anterior chest wall and spread out.
Lymphatic Pumps • Dysfunction: Lymphatic Stasis • Objective: Improve lymphatic flow by altering intrathoracic pressure • Technique: Several different variations, including thoracic and pedal pump
Pedal Pump “Fun With Alex” Lots of good action in this video. Alex is behind the wheel of a Ford F150. There is pumping, driving, revving in sneakers, white socks and barefeet. Alex is a hottie and knows how to pump it
Lymphatic Pump Technique: Thoracic • Place your hands on the patient's anterior chest wall over the patient's pectoralis major muscles. The heels of your hands should lie on ribs 2-4. • With your elbows straight, have the patient breathe in through their open mouth and exhale passively. As the patient exhales, follow the exhalation motion downward and maintain the end point. This applies a compressive force. • With each following breath, slightly resist inhalation and maintain your pressure at the end position of exhalation. • One third of the way through the fourth or fifth inhalation, briskly remove your hands from the chest wall, as a rush of air will enter the patient's lungs.
Pedal Pump • A venous and lymphatic drainage technique applied through the lower extremities • Rhythmic plantar and dorsiflexion of the lower extremities • Physician at foot of patient, patient supine • Rate 30-45 cycles/minute
Kirksville Krunch • Patient Position: Supine • Physician Position: Side of patient, opposite side of posterior transverse process • Patient crosses arms, “opposite over adjacent” • Thenar eminence under posterior transverse process of dysfunctional segment • Patient rolled onto table to the point where flexion is felt at level of dysfunctional segment • Sidebend to engage restrictive barrier • Pt takes deep breath and exhales • At end of exhalation, HVLA thrust is applied straight down to fulcrum (thenar eminence)
Question 1: A 34 year old female comes to the office complaining of mild left sided thoracic pain. The pain started about a week after she began driving a new sports car with very low riding seats. The pain is worse with inhalation. On PE, ribs 3-5 on the left are more caudad and lag behind during inhalation. How would you name the above somatic dysfunction? • Left ribs 3-5 inhalation dysfunction • Left ribs 3-5 exhalation dysfunction • Right ribs 3-5 inhalation dysfunction • Right ribs 3-5 exhalation dysfunction
Question 2 In the previous case, which rib would be the “key rib” through which to direct treatment? • Rib 2 • Rib 3 • Rib 4 • Rib 5 • Rib 6
Question 3 If you choose to treat the previous patient with the “Kirksville Krunch” HVLA, in which direction would the thrust be applied? • Cephalad • Caudad • Straight down towards your fulcrum • HVLA contraindicated in the prior patient because she is a female of child bearing age
"Randy Works the Cavalier" Socks & BarefootRandy is from the midwest and worked his Cavalier in socks and barefoot. There is pumping and driving in this video with some cool angles.