Download
1 / 11
110 likes | 234 Views
Correlation Results Public and Private Sector National Hospital Cost Data Collections (NHCDC). 2013 Activity Based Funding Conference Sydney 15 th May 2013 Dr Brian Hanning Medical Director Australian Health Service Alliance (AHSA). Introduction.

E N D
Correlation Results Public and Private Sector National Hospital Cost Data Collections (NHCDC) 2013 Activity Based Funding Conference Sydney 15th May 2013 Dr Brian Hanning Medical Director Australian Health Service Alliance (AHSA)
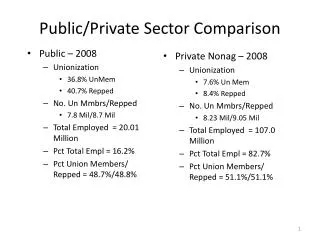
Introduction • AHSA uses a DRG payment model (Equitable Payment Model – EPM) • contains relative weights based on NHCDC private sector data • Some private hospitals have questioned the accuracy of relative weights based on cost modelling • These are based mainly on cost modelling • Further some have asserted that EPM weights are inaccurate compared to public sector weights • These are based mainly on patient level costing • AHSA has investigated these assertions • The implications of the findings are discussed
Hypothesis / Methodology Are the average DRG cost by sector highly correlated over relevant DRGs when cost buckets common to both sectors are considered? • EPM covers acute care type DRGs only • Private sector DRGs with under 30 cases are excluded • Some cost buckets are excluded and others discounted • similar to IHPA discounts of public weights for private cases • Average cost per case for DRGs relevant to EPM were calculated
Modification of Cost buckets Excluded from correlation: • Prostheses • Radiology • Pathology • Interest • Depreciation • Emergency • Ward Medical (There are few HMOs in the private sector) Public Sector Costs Discounted in correlation : • These discounts reflect medical costs in public sector cost buckets, consistent with IHPA methodology • Critical Care by 15% • Theatre and Special Suite by 37.5%
NHCDC Studies correlated • Average costs were correlated for each of the three most recent NHCDC where results were available for both sectors • Rounds 11 (2006-7) to Round 13 (2008-9) all based on ARDRGv5 • all these studies appeared robust • Correlation is between average cost by DRG over the two sectors based on relevant cost buckets for ~600 DRGs • does not reflect absolute cost differences at the DRG level between the two sectors • No private sector NHCDC ARDRGv6 study has made publicly available to date
Results - 1 Table 1 – Correlation of average DRG cost between the public and private sectors
Results - 2 Table 2 – Correlation between various NHCDC studies
Public Private Correlation • Consistently high correlation between public and private studies • cross validates both studies • A presentation noting high correlation between public and private sector studies was given at the 2000 Casemix Conference • EPM was in development at about that time B. Hanning, “Can Private Sector Cost Weights be appropriately based on the National Cost Data Collection – Private Sector?”, Conference Proceedings the 12th Casemix Conference in Australia, Cairns, 28th to 30th August 2000. p 331-332 Conclusion • Private sector NHCDC is an appropriate basis for deriving private sector weights • EPM weights include all relevant cost buckets to the private sector • Concerns about the use of cost modelling at the DRG level are not well based. • In principle the public sector NHCDC weights could be used to derive robust private sector weights although not the converse
AHSA Policy: Correlation NHCDC Studies • If cost weights are highly correlated between the most recent study and the study in which EPM weights are based: • AHSA does not change weight versions. • threshold for change is under 85% correlation • saves both hospitals and funders time and expense • Correlation between the three ARDRGv5 based NHCDC studies exceed the 85% threshold • Should IHPA have a similar policy in the public sector? • A danger of this policy – cessation of annual NHCDC studies • High correlation can only be confirmed by annual studies • The loss of corporate knowledge will impair the quality of biannual or less frequent studies
Conclusion • Well based private sector NHCDC studies are an appropriate basis for deriving relative DRG weights • The high correlation of public and private sectors is a significant cross validation of both studies • It is not significant that the private sector study is generally based on cost modelling rather than patient level costing