Download

1 / 79
820 likes | 975 Views
Surgical Care Improvement Project. Dr. Philmore J. Joseph Memorial Hermann NE Humble, Texas. "It may seem a strange principle to enunciate as the very first requirement in a hospital that it should do the sick no harm" Florence Nightingale .

E N D
Surgical Care Improvement Project Dr. Philmore J. Joseph Memorial Hermann NE Humble, Texas
"It may seem a strange principle to enunciate as the very first requirement in a hospital that it should do the sick no harm" Florence Nightingale
Nosocomial infection =Any infection that is not present or incubating at the time the patient is admitted to the hospital
History of infection control and hospital epidemiology • Pre 1800: Early efforts at wound prophylaxis • 1800-1940: Nightingale, Semmelweis, Lister, Pasteur • 1940-1960: Antibiotic era begins, Staph. aureus nursery outbreaks, hygiene focus • 1960-1970’s: Documenting need for infection control programs, surveillance begins • 1980’s: focus on patient care practices, intensive care units, resistant organisms, HIV • 1990’s: Hospital Epidemiology = Infection control, quality improvement and economics • 2000’s: ??Healthcare system epidemiology modified from McGowan, SHEA/CDC/AHA training course
History of infection control and hospital epidemiology • Pre 1800: Early efforts at wound prophylaxis • 1800-1940: Nightingale, Semmelweis, Lister, Pasteur • 1940-1960: Antibiotic era begins, Staph. aureus nursery outbreaks, hygiene focus • 1960-1970’s: Documenting need for infection control programs, surveillance begins • 1980’s: focus on patient care practices, intensive care units, resistant organisms, HIV • 1990’s: Hospital Epidemiology = Infection control, quality improvement and economics • 2000’s: ??Healthcare system epidemiology modified from McGowan, SHEA/CDC/AHA training course
Medicare Surgical Infection Prevention (SIP) Project Objective To decrease the morbidity and mortality associated with postoperative infection in the Medicare patient population
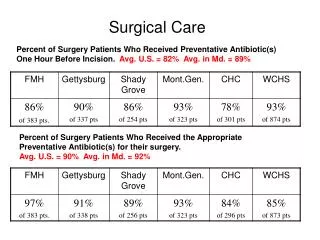
Infected Un-infected Mortality 7.8% 3.5% ICU admission 29% 18% Length of Stay 11 days 6 days Median direct cost $7,531 $3,844 Readmission 41% 7% Surgical Infection PreventionPerformance Stratified by Risk Class Kirkland. Infect Control Hosp Epidemiol. 1999;20:725.
American College of Surgeons American Hospital Association American Society of Anesthesiologists Association of peri-Operative Registered Nurses Agency for Healthcare Research and Quality Centers for Medicare & Medicaid Services Centers for Disease Control and Prevention Department of Veteran’s Affairs Institute for Healthcare Improvement Joint Commission on Accreditation of Healthcare Organizations SCIP Steering Committee
Surgical Care Improvement Project(SCIP) • Preventable Complication Modules • Surgical infection prevention • Cardiovascular complication prevention • Venous thromboembolism prevention • Respiratory complication prevention
Surgical Care Improvement Project(Draft Global Outcome Measures) • Motality within 30 days of surgery • Readmission within 30 days of surgery
Surgical Care Improvement ProjectPerformance measures • Surgical infection prevention • Antibiotics • Administration within one hour before incision • Use of antimicrobial recommended in guideline • Discontinuation within 24 hours of surgery end • Glucose control in cardiac surgery patients • <200 gm/dl at 6am postoperatively • Proper hair removal • Normothermia in colorectal surgery patients • Immediate postoperative • SSI rates during index hospitalization (test outcome)
Perioperative AntibioticsTiming of Administration 14/369 15/441 1/41 1/47 1/81 2/180 5/699 5/1009 Hours From Incision Classen, et al. N Engl J Med. 1992;328:281.
Pre-operative shaving • Shaving the surgical site with a razor induces small skin lacerations • potential sites for infection • disturbs hair follicles which are often colonized with S. aureus • Risk greatest when done the night before • Patient education • be sure patients know that they should not do you a favor and shave before they come to the hospital!
Perioperative Glucose Control • 1,000 cardiothoracic surgery patients • Diabetics and non-diabetics with hyperglycemia Patients with a blood sugar > 300 mg/dL during or within 48 hours of surgery had more than 3X the likelihood of a wound infection! Latham R, et al. Infect Control Hosp Epidemiol. 2001.
Perioperative Glucose Control Carr J Thor Surg 2005
Temperature Control • 200 colorectal surgery patients • control - routine intraoperative thermal care (mean temp 34.7°C) • treatment - active warming (mean temp on arrival to recovery 36.6°C) • Results • control - 19% SSI (18/96) • treatment - 6% SSI (6/104), P=0.009 • Measure: Colorectal surgery patients with immediate postoperative normothermia Kurz A, et al. N Engl J Med. 1996. Also: Melling AC, et al. Lancet. 2001. (preop warming)
Surgical Care Improvement ProjectDraft performance measures • Perioperative cardiac events • Surgery patients on a beta-blocker prior to arrival that received a beta-blocker during the perioperative period Perioperative is defined as preoperatively on the day of surgery or intraoperatively prior to extubation.
6-month survival 100% vs 92% (P<0.001) 2-yr survival 90% vs 79% (P=0.019) Postoperative Survival Mangano DT, et al. N Engl J Med. 1996;335:1713-20.
Potential to Reduce Perioperative Complications in SCIP Based on the goal of achieving near-complete guideline compliance to prevent each of these complications as compared to current national rates of guideline compliance for each complication.
Crossing the Quality Chasm “In its current form, habits, and environment, the health care system is incapable of giving Americans the health care they want and deserve….The current care systems cannot do the job. Trying harder will not work. Changing systems of care will.”
Adopter Categories Innovators Early Majority Late Majority Early Adopters Laggards 34% 2.5% 13.5% 34% 16% from E. Rogers, 1995
What is Six Sigma? • A comprehensive and flexible program for achieving, sustaining and maximizing business success that: • Is uniquely driven by a clear focus on the “Voice of the Customer” • Is founded in a rigorous use of facts, data and statistical analysis • Provides for diligent attention on managing, improving and reinventing business processes. • Is an management methodology with three perspectives: • A Measure of Quality • A Process for Continuous Improvement • An Enabler for Cultural Change
A Measure of Quality: • Six Sigma is a statistical measure that expresses how close a service process comes to its quality goal • Six Sigma refers to a process that produces only 3.4 defects per million opportunities
A Process for Continuous Improvement: • Six Sigma provides a process based approach (DMAIC) to continuous improvement that can be used to improve any business process • Provides a data driven and evidence based format on which to base improvement decisions • Insists on statistical proof of improvement and process control • Provides a means to sustain and build upon proven improvements
Six Sigma Themes: • Genuine Focus on the customer • Data and Fact Driven Management • Process focus, management and improvement • Proactive management • Boundaryless collaboration • Drive for perfection; tolerance for failure
Six Sigma Methodology Change Acceleration Process Effective Results Work-OutTM Six Sigma Effectiveness: The Effectiveness (E) of the result is equal to the Quality (Q) of the solution times the Acceptance (A) of the idea. Q x A = E
Keys To Physician Acceptance • Credible evidence based literature • Evidence should be compelling • Presented by a credible, respected physician (preferably their specialty) • Explain that their peers endorse
Hospital Process In Place To Educate Physicians • EBM education to medical staff • Process to help physicians with indicators • Concurrent review to catch missed indicators (early, late) • Retrospective review (educational) • Physician profiles
Rationale to Support Physician/Hospital Compliance • Right thing to do • Quality issue • Financial issue(P4P) • Liability issue • Public reporting issue • Need to hold physician accountable (only if hospital has process in place)
SCIP 1 – Barriers(Antibiotic Within One Hour) • Never gets done in one hour • Doesn’t make any difference • No infections • Never use antibiotics anyway
SCIP 1 – Responses (Antibiotic Within One Hour) • Literature clear (EBM) • Does make a difference • Infections are related to timing of 1st dose • Antibiotics are effective • Hospital process (delegate individual/ team) • Tourniquet issue • Vancomycin issue
SCIP 2 – Barriers(Evidence Based Antibiotic) • Who are these experts telling me (30 years experience) what to do? • Are they clinically involved, on the “battlefield” like me? • My patients don’t get infections. • Don’t tell me how to practice medicine/surgery.
SCIP 2 – Barriers, cont’d(Evidence Based Antibiotic) • Why can’t I use Vancomycin on all my patients? • Why can’t I use antibiotic “x” • FDA approved • Endorsed by manufacturer
SCIP 2 – Responses (Evidence Based Antibiotic) • Experts are knowledgeable, credible, and in active practice. • You have been lucky so far (won’t be able to defend SSI with unapproved antibiotic). • Vancomycin over utilized • Increased infection rates • Increased resistance
SCIP 2 – Responses, cont’d (Evidence Based Antibiotic) • Many antibiotics approved by FDA, and manufacturer endorsed, not agreed by experts as good prophylaxis at this time (inadequate trials, time)
SCIP 3 – Barriers(Why Physicians Don’t Stop ABX at 24 Hours) • Most difficult • Just because • Fever • Infection • Tubes, drains, still in place
SCIP 3 – Barriers, cont’d(Why Physicians Don’t Stop ABX at 24 Hours) • No literature to support • My patients are sicker • Training program taught me this way • I know what is best for my patient
SCIP 3 – Responses(Why Physicians Don’t Stop ABX at 24 Hours) • Ample literature to support (many years). (one drug, one dose, one time, many procedures) • Fever usually secondary to atelectasis. • If infection on prophylactic ABX, no sense to continue (?resistance). • Contact surgical training program.
SCIP 3 – Responses, cont’d(Why Physicians Don’t Stop ABX at 24 Hours) • You may not know what is best for your patients (only your assumption). • Meet with ACS state chapters. • Meet with medical school surgical programs. • Society of Thoracic Surgery 48 Hours