Download
1 / 22
270 likes | 905 Views
Vortex Keratopathy. 68 year old female Chief complaint: Blur at near in OD>OS Dryness OU Medical Hx: Allergies Hypertension Irregular Heart Beat. Exam Findings. PERRL (–)APD EOM: Full and Smooth CF: FTFC

E N D
Vortex Keratopathy • 68 year old female • Chief complaint: Blur at near in OD>OS Dryness OU • Medical Hx: Allergies Hypertension Irregular Heart Beat
Exam Findings • PERRL (–)APD • EOM: Full and Smooth • CF: FTFC • Rx: OD: +1.50-1.00x085 OS: -0.50-1.25x100 OU: +2.25 Add • VA: 20/40 OD, 20/20 OS @ D/N
Slit Lamp Exam OD OS • Lids/Lashes: Clear Clear • Conjunctiva: Clear Clear • Cornea: INFERIOR WHORLS • Anterior Chamber: D&Q D&Q • Iris: Clear Clear • IOP: 16mmHg OU
Fundoscopy OD OS • Lens NS2, PSC 1+ PCIOL • C/D .2/.2 .2/.2 • A/V 2/3 2/3 • Macula Clear Clear • Vitreous PVD PVD • Periphery (-)Breaks/Tears
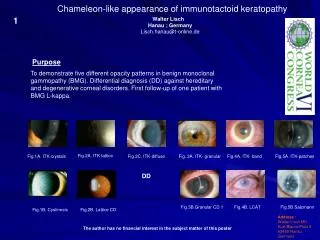
Corneal Verticillata • Whorl-like pattern of yellow or brown deposits confined to the inferior central cornea. • At the level of the deep epithelium(50microns). • Limbal-sparing. • Delineate epithelial migration patterns.
Etiology • Fabry’s disease. • Reaction to systemic drug therapy including: Amiodarone Chloroquine Indomethacin Chlorpromazine Tamoxifen
Fabry’s Disease • Fabry's disease is an X-linked recessive lipid storage disorder with an incidence of about 1 in 40,000. • Deficiency of the enzyme alpha-galactosidase A results in the accumulation of ceramide trihexoside. • Symptoms include skin lesions and neurologic changes. Painful neuropathy is common; often associated with a low-grade fever. • Hypohydrosis is common and can lead to heatstroke.
Fabry’s Disease • Deposits of lipid in the myocardium can lead to arrhythmia, myocardial infarction and valvular dysfunction. Involvement of small cerebral vascular vessels can result in cerebral hemorrhage. • Deposits of lipid in the kidney can lead to progressive renal compromise and renal failure. • Confirmation with a blood test: Alpha-galactosidase level (Normal range is 19 to 29).
Fabrys’ Disease and the Eye • Corneal verticillata. • Conjunctival and retinal vessel tortuosity. • Oculomotor abnormalities. • Anterior subcapsular cataracts. • Periorbital edema.
Amiodarone • Amiodarone hydrochloride is a Class III antiarrhythmic agent. • Usual dose is 200-600mg/ day. • Prolongs the action potential duration and refractory period of atrial, nodal and ventricular tissues. • Amiodarone increases coronary blood flow, decreases cardiac oxygen requirements and also suppresses ectopic pacemakers.
Amiodarone and the Eye • Corneal verticillata. • Decrease in vision, rarely. • Photophobia. • Colored halos. • Dyschromatopsia. • Dry eye. • Anterior ischemic optic neuropathy*.
As it turns out… • Patient has ocular dryness, and anterior subcapsular cataract. • This patient has been on Amiodarone for several years for her heart arrhythmia. • *Color vision testing may be helpful if medical history is unreliable.
Mechanism of Keratopathy • Amphiphilic drugs; amiodarone, chloroquines and phenothiazones deposit verticillata. • Verticillata form when drug complexes with phospholipids in the cells. • Complexes cannot be metabolized by lysosomal phospholipases and remain within the cornea.
Amiodarone Keratopathy • Grading System • 1- Small, brown punctate epithelial opacities within inferior temporal cornea arranged in a single line. • 2- Branching pattern to line of opacities. • 3- Increase in branches to form a whorl. • 4- Whorling with irregular clumps of brown pigment.
Amiodarone and AION • Patients on Amiodarone have a severe cerebrovascular deficit. An AION is most likely due to the illness rather than a reaction to the drug.
Studies… • Most studies suggest that all taking Amiodarone will develop verticillata. • Journal of AOA, 1985. Observations of 21 patients on a daily dosage of 200-600 mg for periods ranging from six months to three years. Corneal deposits developed in all 21 patients and anterior lens opacities developed in 12 of 20 phakic patients.
Studies… • Cornea, 2001. Eleven patients on amiodarone therapy were observed. All patients showed the presence of high reflective, bright intracellular inclusions in the epithelial layers.
Studies… • Cardiology No.5, 2003. Examination of 298 patients who received oral amiodarone for 1–122 months (mean 27,3±1,5 months). • Signs of keratopathy were found in 280 patients (94%). Severity of keratopathy depended on cumulative drug dose and duration of administration.
Studies… • Digital Journal of Ophthalmology, 2004. • Evaluated Amiodarone Keratopathy using the computer operated corneal topographers. • Corneal topography of 7 of 8 eyes revealed an unusual irregular astigmatism with generalized mild inferior temporal steepening consistent with the location of the corneal deposits. • Note: LASIK or PRK are not recommended.
Treatment • There is no recommended treatment for verticillata. • Medication regimens are not altered based on the presence of corneal deposits. • If drug is stopped, most verticillata will eventually disappear within seven months. • Unknown history warrants investigation!