Download
1 / 26
270 likes | 567 Views
Protozology (proto = primitive) Study of protozoa. Blood flagellates ( Haemoflagellates ) 1. African Trypanosomiasis (Sleeping sickness) 2. American Trypanosomiasis ( Chagas disease) 3. Leishmaniasis. Blood sorozoans : Malaria (Plasmodium) Toxoplasmosis.

E N D
Protozology (proto = primitive) Study of protozoa • Blood flagellates (Haemoflagellates) • 1. African Trypanosomiasis (Sleeping sickness) • 2. American Trypanosomiasis (Chagas disease) • 3. Leishmaniasis • Blood sorozoans: • Malaria (Plasmodium) • Toxoplasmosis
Blood flagellates (Haemoflagellates) Are hemoflagellates protozoan belonging to Zoomastigophorai.e. Move by flagella and divide by longitudinal fission 1. Trypanosoma gambiense & Trypanosoma rhodesiense: African trypanosomiasis. 2. Trypanosoma cruzi: American trypanosomiasis (Chagas disease). 3. Leishmania donovani: Visceral leishmaniasis (kala-azar) 4. Leishmania tropica: Cutaneous leishmaniasis (oriental sore) 5. Leishmania braziliensis: Mucocutaneous leishmaniasis (Espundia)
American trypanosomiasis (Chagas disease). African Trypanosomiasis (Sleeping sickness) Caused by Trypanosoma cruzi • Caused by Trypanosoma gambiense (west African) and Trypanosoma rhodesiense (East African).
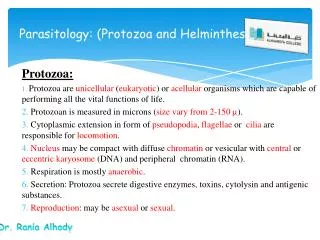
African American by bugs e.g. Triatoma infestans. The bug releases trypomastigotes in its feces near the wound, which enter the host throughthe wound or through intact mucosal membranes Habitat The infection by Tse tse fly. The metacyclic trypanosomal forms in the saliva of the insect are inoculated to human during the bite. Morphology Trypanosoma appear in the peripheral blood 5 to 21 days after the infecting bite. Trypanosomacruzi in blood sample, Giemsa stained Trypanosoma, 18-30 µm in length, in peripheral blood. Giemsa stain
African Trypanosomiasis (Sleeping sickness) Clinical findings: Infection occurs in 3 stages. 1-Trypanosomal primary lesion (chancre) develops at the site of bite (the parasite multiply). 2-Hemolymphatic early stage where the parasite reach and multiply in blood with fever, sweating, headache, anemia, increased pulse rate, joint and muscle pain and enlarged regional lymph nodes (lymphadenopathy). 3-Cerebral late stage where the parasite reach the C.N.S. causing chronic inflammation with ischaemia and hemorrhage leading to meningoencephalitis, with sever headache, mental dullness and excessive sleeping, finally coma and death. Treatment Suramin or Pentamidine for hemolymphatic stage and melarsoprol for late cerebral stage. Laboratory diagnosis Microscopic examination - ELISA.
American trypanosomiasis (Chagas disease) Clinical findings • A local lesion (chagoma) can appear at the site of inoculation. • The acute phase is usually asymptomatic, but can present with manifestations that include fever, anorexia, lymphadenopathy, mild hepatosplenomegaly, and myocarditis. • Most acute cases resolve over a period of 2 to 3 months into an asymptomatic chronic stage. The symptomatic chronic stage may not occur for years. Its manifestations include cardiomyopathy (the most serious manifestation); pathologies of the digestive tract (megacolon) and weight loss. Chronic Chagas disease and its complications can be fatal.
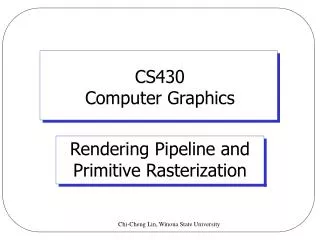
American trypanosomiasis Chagoma Chancre African trypanosomiasis
Laboratory diagnosis • Microscopic examination of fresh anticoagulated blood for motile trypanosomes with Giemsa. • ELISA for detection of specific antibody in chronic Chagas disease. • Culture on diphasic Novy-Nicholle-MacNeal’s (NNN) medium • Xenodiagnosis, where uninfected bugs are fed on the patient's blood, and their gut contents examined for parasites 4 weeks later. Treatment • Must be initiated early and not delayed for results of isolation of the parasite. • The drug of choice is benznidazole but once the disease has progressed to later stages, no medication has been proven to be effective.
LeishmaniasisZoomastigophora Leishmania donovani : Visceral Leishmaniasis (Kala-azar) Leishmania tropica : Cutaneous Leishmaniasis (Tropical sore) Leishmania braziliensis: MucocutaneousLeishmaniasis (Espundia) Leishmaniasis is found in parts of about 88 countries. Approximately 350 million people live in these areas. Cutaneous leishmaniasis is found in Egypt Leishmania tropica
Habitat Transmision by sand flies Mode of infection: inject the infective stage (promastigotes) during blood meals, which are phagocyted by macrophages and transform into amastigotes, which multiply in infected cells and affect the internal organs (visceral leishmaniasis), Disease: Skin (cutaneous leishmaniasis), or mucocutaneous tissue and skin (mucocutaneous leishmaniasis). Leishamnia amastigotes, bone marrow aspirate, Giemsa stain Leishamnia promastigotes having a single flagellum, Giemsa stain
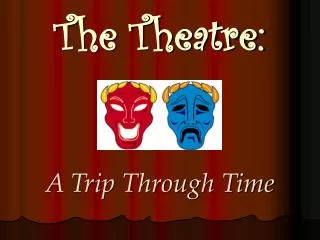
Clinical findings • Cutaneous leishmaniasis is characterized by one or more cutaneous lesions on areas where sand flies have fed, which finally ulcerate and discharge thin, offensive pus. It heals within months leaving depigmented scare. Ulcers often end up looking somewhat like a volcano, with a raised edge and central crater. Leishmania tropica • Mucocutaneous leishmaniasis shows similar lesion but affect mucus membranes causing destruction of bone & cartilage of nose and mouth Leishmania braziliensis • Visceral leishmaniasis (kala-azar) usually cause fever, weight loss, and an enlarged spleen and liver. Patients usually have dark skin specially forehead and around mouth. Leishmania donovani Laboratory diagnosis • Microscopic examination with Giemsa stain • Culture on diphasic NNN medium • ELISA Treatment Pentavalent antimony compounds or sodium stibogluconate (under investigation).
cutaneous leishmaniasis Mucocutaneous leishmaniasis Visceral leishmaniasis
Blood sorozoans: Sporozoasida Malaria (Plasmodium) • Plasmodium vivax(Benign tertian malaria) • Plasmodium ovale(Ovale tertian malaria) • Plasmodium malariae (Quartan malaria) • Plasmodium falciparum(Malignant tertian malaria)
Habitat • The malaria parasite life cycle involves two hosts. A female Anopheles mosquito (the definitive host) transmits a motile infective form (called the sporozoite) to a vertebrate host such as a human (the secondary host) Note:Wuchereria bancrofti vector is Anopheles mosquito also • It inoculates sporozoites into the human, which matures to schizonts in liver cells and release merozoites into the blood stream.
Clinical findings 1- Malarial classical symptoms release of merozoites and their toxin from ruptured RBCS in the end of each erythrocytic cycle which complete every 72 hours in Plasmodium malariaeand every 24 hours in other species: it consists of a- Cold stage or rigor stage (10 min to one hour) b- Hot or fever stage (1-4 hours), due to release of most merozoites. c- Sweating stage (1-4 hours), due to rapid drop of temp and is accompanied by reinfection of RBCs. 2-Anemiadue to destruction of RBCs, splenomegaly and hepatomegaly due to engulfed pigment by R.E.S. 3- Adhesion and clumping of infected RBCs in capillaries cause their occlusion (thrombocytopenia) , headache, myalgia, convulsions, coma, diarrhea or dysentery and dehydration.
Laboratory diagnosis • Blood film (thin and thick films) for comparison of Plasmodium species • Serological reaction (ELISA) when detection of the parasite is difficult. • Treatment • Quinine and chloroquine for blood forms. • Primaquine & pyrimethamine for hepatic forms.
Toxoplasmosis • Caused by Toxoplasma gondii • Disease toxoplasmosis. • Congenital toxoplasmosis being the most serious form of human infection. • It has a worldwide distribution. Habitat • It is an obligate intracellular parasite that invade all cells except RBCs (non-nucleated). • Infection is usually mild, may be chronic or acute. • Severe infection is being seen increasingly often in the immuno-compromised host undergoing immunosuppressive therapy for malignancies or organ transplants.
Morphology • Pseudocysts:Intracellular collection of trophozoites in macrophages and R.E.S. cells. • Trophozoite (tachyzoite):Intracellular, crescent shaped with central nucleus • Cysts:collection of trophozoites enclosed in a tissue cyst formed in chronic stage or latent infection when immunity develops. • Oocysts: Oval, contain 2 sporocysts each containing four sporozoites and found in stool of infected cats.
The sexual part of the life cycle takes place only in cats, which makes cats the parasite's primary host. The second asexual phase, can take place in other warm-blooded animals, including cats, mice, humans, and birds. The hosts in which asexual reproduction takes place is the intermediate host.
Modes of transmission: • ingestion of undercooked infected meat containing Toxoplasma cysts • B) ingestion of the oocyst from fecally contaminated hands or food • C) organ transplantation or blood transfusion; • D) transplacental (congenital) transmission,
Clinical findings • Acquired: • Most healthy people who acquire toxoplasma infection do not experience any significant symptoms, however about 10% of people develop a mild to moderate self limiting flu-like or glandular fever-like illness. Lymphadenopathy (enlarged regional lymph nodes) is the most common manifestation, lasting up to 4-6 weeks but fatigue, sore throat, myalgia, (or, very rarely, rashes, arthralgia or hepatosplenomegaly) may occur. In rare cases symptoms may persist for many months or years and may be due to chronic active infection. Serious or fatal infection occurs in immunodeficiency as in AIDS.
2. Congenital toxoplasmosis: Cause severe, often fatal cerebral damage to a fetus and who recover often show mental defects. In early pregnancy it cause abortion or still birth and in late pregnancy symptoms occur in the infant 2-3 months after birth.
Laboratory diagnosis 1. Microscopic examination of aspirates and fluids. 2. ELISA. 3. Animal inoculation (e.g. lymph node biopsy material in mice). Treatment: • Treatment is not needed for a healthy person who is not pregnant, as the infection is usually self limiting. • Treatment with sulphadiazine and pyrimethamine or trimethoprime, may be recommended for pregnant women or persons who have weakened immune systems.