Download
1 / 24
350 likes | 3.3k Views
Sarah Carney & M. Chowdhury FY1 CMFT 5 th Yr Finals Revision Day. Hernias & Stomas: OSCE Finals. Predisposing factors and Presentation:. Predisposing factors: Chronic cough (smoking) Chronic constipation Straining to pass faeces Straining to void Obesity Increasing age Surgery

E N D
Sarah Carney & M. Chowdhury FY1 CMFT 5th Yr Finals Revision Day Hernias & Stomas: OSCE Finals
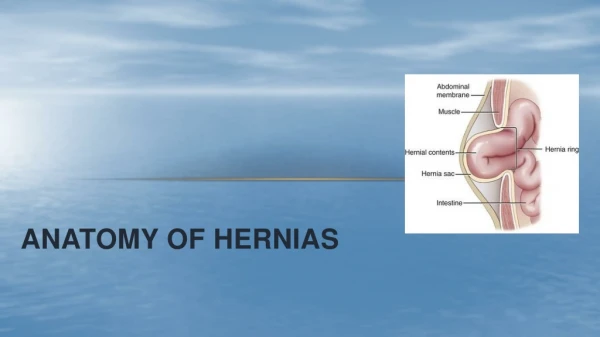
Predisposing factors and Presentation: • Predisposing factors: • Chronic cough (smoking) • Chronic constipation • Straining to pass faeces • Straining to void • Obesity • Increasing age • Surgery • Prostatic disease • Ilioinguinal nerve damage • Occupation/heavy lifting • Presentation: • Lump • Pain • Complication: obstruction, strangulation
Classification of hernias • Congenital and acquired • Abdominal and extra-abdominal • Groin hernias • Inguinal: direct and indirect • Femoral • Inguinal scrotal
Femoral hernias: • Femoral canal: • Position: BELOW and LATERAL to pubic tubercle • Borders of femoral ring: • Medial: lacunar ligament (↑strangulation) • Anterior: inguinal ligament • Posterior: pectineal ligament and pectineus • Lateral: femoral vein • Management: • Elective: low approach: excision of the sac (herniotomy) and repair (herniorraphy): suture inguinal to pectineal ligament • Emergency: high approach: similar but done through the abdominal wall?/nguinal canal to assess plus/minus resect bowel
Hernias: Inguinal: Anatomy • Boundaries • Superior: fibres of transversalis, internal oblique and conjoint tendon medially • Inferior : inguinal ligament and lacunar ligament medially • Anterior: external oblique aponeurosis and internal oblique for the lateral third , superficial ring medially • Posterior : laterally transversalis fascia including deep inguinal ring, medially conjoint tendon • Contents of inguinal canal: • Males: spermatic cord and ilioinguinal nerve • Females: round ligament and ilioinguinal nerve
Inguinal hernias: direct and indirect Deep inguinal ring: hole in transversalis fascia (midpoint of the inguinal ligament) Superficial ring: hole in external aponeurosis, found above and medial to pubic tubercle
Assessing for direct or indirect hernia: • Reduce the hernia • Apply pressure with a finger over the deep inguinal ring • 1.5cm above midpoint of inguinal ligament (ASIS to pubic tubercle) • NB: midinguinal point (ASIS to pubic symphysis): femoral artery • Ask patient to cough/strain • If controlled, probably indirect. If not controlled, probably direct hernia
Differential diagnoses lumps in the groin: • Inguinal lymph node/lymphadenopathy • Saphena varix: dilated vein at SFJ which disappears on lying flat • Femoral artery aneurysm • Encysted hyrocele of the cord • Lipoma of the cord • Incompletely descended testicle • Hernia: inguinal, inguinal scrotal, femoral • Psoas abscess
Management of hernia: • Investigation: USS, MRI scan • Conservative: treatment of causes, truss • Surgical: • open approach (GA/LA/regional) • Laparoscopic: define anatomy, inspect and excise hernial sac, close the defect (tension-free) • Herniorraphy: suture the defect (shouldice repair) • Hernioplasty: prosthetic mesh (lichtenstein mesh tension-free repair)
Other hernias • Incisional hernias • Umbilical hernias: mayo repair • Richter’s: only part of the circumference of the bowel is within the sac. Can strangulate without obstruction • Epigastric: through linea alba • Spigelian: through arcuate line of douglas (where posterior rectus sheath becomes deficient) • Obturator: thin old ladies
Examination of Hernia • Introduction, Inspection, Palpation, Percussion, Auscultation • Intro: • Introduce, explain, consent, exposure, chaperone, patient name and DOB. • Ask about pain, fever, bowel movements • Exposure: abdomen, groin, legs.
Inspection • Ask patient to stand up • Inspection: • Lumps/swellings • Scars (surgery predisposing factor for hernias) • Skin changes over hernia (redness/shinyness): suggestive of acute inflammation/strangulation • Tenderness/ redness/ swelling • Unilateral or bilateral swellings. • Does the lump extend into the scrotum • Describe the shape and size when hernia is fully distended (ask patient to cough): • Pyriform shape of indirect hernia • Globular shape of direct hernia • Any other scrotal swellings/ Previous operation scars • Describe the position of the swelling: • Inguinal hernias above and medial to pubic tubercle • Femoral hernias below and lateral to pubic tubercle
Palpation • Palpate for: • Temperature • Tenderness • Size and shape • Consistency • For inguinal scrotal swellings: • confirm that it is not possible to get above the swelling • Palpate the testes and see if the hernia stops above the testis (acquired hernia) or incorporates the testis (congenital) • See if hernia is reducible • Tests for distinguishing indirect from direct inguinal, and for distinguishing inguinal from femoral
Differentiating between inguinal and femoral hernia: • Find pubic tubercle • Reduce the hernia • Ask patient to cough • See if and where hernia re-emerges: above and medial inguinal. Below and lateral femoral.
To complete the examination: • Auscultate over any hernia: bowel sounds if hernia is enterocele. Otherwise, auscultation is of no diagnostic value • Other tests/ examinations:Examine patient on lying down: • Direct hernia usually reduces by itself on lying down (unless strangulated) • Indirect hernia usually requires manual reducing • Hydrocele reduces over several hours of sleep • Examine the abdomen (and possible the respiratory system for evidence of chronic cough, e.g. chronic bronchitis or TB, etc.) • Examine the testicles. To differentiate a hernia from a testicular swelling. Test this by seeing if you can get your fingers above the testicular swelling. With a testicular swelling you will, with a hernia, you won’t. • Examine scrotum, cord, testes of both sides. Need to confirm contralateral side is normal. • Perform a DRE to see if prostate is enlarged straining. Commonest cause for direct hernias in the elderly • Examine and take a history to assess the risk factors.
Stomas: • Colostomy: surgical procedure that involves connecting part of the bowel onto the anterior abdominal cavity. Patient has an opening on the abdomen: stoma. • Permanent or temporary • Urostomies • http://www.allaboutbowelsurgery.com/shared/stoma_care/stoma_surgery/
Examination of stoma • Site • Calibre – thin/wide • Number of lumens • Functioning/healthy? • Colour/surface • Bag: contents, surrounding skin • Contact dermatitis/blisters • Any parastomal hernia • Inspect perineum
Complications of stomas: • Anatomical and metabolic • Early and late • Metabolic: • Renal calculi • Electrolyte imbalance • Psychological/psychosexual • Anatomical: • Parastomal hernia • Prolapse of ileostomies • Parastomal dermatitis