Download

1 / 83
830 likes | 836 Views
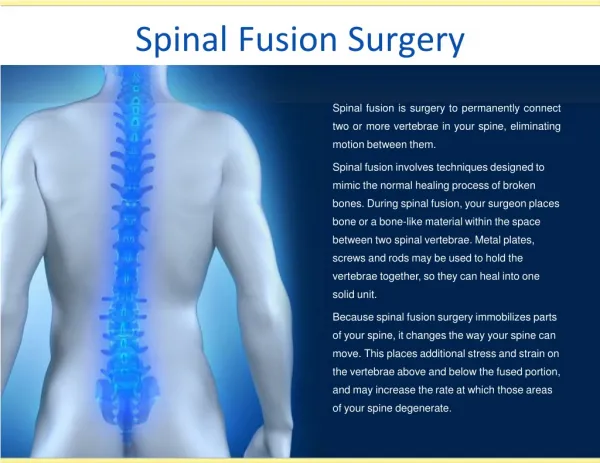
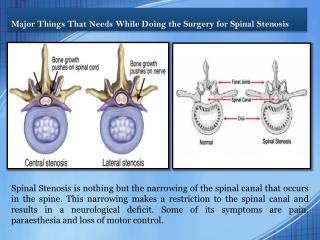
The Spine is an integral part of the human body that protects our spinal cord and supports our body weight. A healthy spine is made up of multiple small bones called vertebrae that are stacked on top of each other with fibrous discs placed in between them.

E N D
The importance of the sagittal profile inspinal deformitysurgery Jwalant S.Mehta FRCS (Orth), MCh (Orth), D (Orth), MS(Orth) Consultant Spine DeformitySurgeon The Royal Orthopaedic Hospital, Birmingham Childrens’Hospital BMIHealthcare SpireHealthcare Jwalant S.Mehta www.mehtaspine.com
Outline • Understanding & measuring the sagittalprofile • Pathological changes in sagittalprofile • Surgical reconstruction options • Clinical evidence /cases Jwalant S.Mehta www.mehtaspine.com
Sagittal plane: divides into right & lefthalves t S.Mehta Jwalan www.mehta spine.com
Balance: Head overheels! Jwalant S.Mehta www.mehtaspine.com
The spinal‘fingerprint’ Jwalant S.Mehta www.mehtaspine.com
Cone ofeconomy J.Dubousset Jwalant S.Mehta www.mehtaspine.com
Sagittal PlaneAlignment… … More Than Just theSpine Thoracickyphosis Lumbarlordosis Pelvicmorphology/ version Global Alignment Lowerextremity Jwalant S.Mehta www.mehtaspine.com Biospace /LBM
Sagittal verticalaxis Jwalant S.Mehta www.mehtaspine.com June2014
Jwalant S.Mehta www.mehtaspine.com June2014
Radiographicmeasures Jwalant S.Mehta www.mehtaspine.com
Thoracic kyphosis: 38° ±18 Lumbar lordosis: 48° ±18 Jwalant S.Mehta www.mehtaspine.com
TLJunction T10 L2 Jwalant S.Mehta www.mehtaspine.com June2014
Pelvicmeasures • Sacral slope(SS) • Pelvic tilt(PT) • Pelvic incidence(PI) Jwalant S.Mehta www.mehtaspine.com June2014
Sacralslope • Horizontal & cranial sacral end platetangent • 41°±8.4° (Vialle JBJS2005) Jwalant S.Mehta www.mehtaspine.com
Pelvictilt • Verticalline between • middle of cranial sacralend plate • centre of the bicoxo-femoral • axis • 13° ± 6° (Vialle JBJS2005) Jwalant S.Mehta www.mehtaspine.com
Significance of pelvictilt • Centre of gravity overLL • Maintains sacral plate posterior to the hip • Increases withage Jwalant S.Mehta www.mehtaspine.com
Pelvicincidence • Keyparameter • Perpendicularto: • the middle of the sacralend • plate • mid-point of femoral heads • 55° ± 10.6° (Vialle JBJS2005) Jwalant S.Mehta www.mehtaspine.com
Spino-pelviccompensation • PI regulatesPT • HigherPI Bettercompensation Jwalant S.Mehta www.mehtaspine.com June2014
Jwalant S.Mehta www.mehtaspine.com June2014
PI=PT+SS Jwalant S.Mehta www.mehtaspine.com June2014
Curvetypes Schwab et al. SPINE2011 Modifiers Jwalant S.Mehta www.mehtaspine.com June2014
The sagittal planedeformity Jwalant S.Mehta www.mehtaspine.com June2014
The coronal planedeformity Jwalant S.Mehta www.mehtaspine.com June2014
Spino-pelvic pathologypatterns Progressivekyphosis Gravity line drifts forwards Pelvis rotates backwards Sacral slopedecreases Kneeflexion JwalantS.Mehta www.mehtaspine.com
Type1:Non-harmoniousspine Thoraco lumbardisc Junctionallisthesis Eurospine2007 Bruxelles .Mehta ine.com JwalantS www.mehtasp Ju
Type 2: Harmonious but FlatBack Early discdegeneration lant S.Me htaspine.c Jwa www.me hta om
Type 3:The mostharmonious (“probably a goodback”) Jwalant S.Mehta www.mehtaspine.com
Type 4: Harmonious buthyper-curved. • When young: verystrong • HighPI • Goodlordosis • Withaging • will loselordosis • pelvic tilt increases to compensate foranterior imbalance Lumbarstenosis+spondylolisJwtahlanetSs.Mieshta www.mehtaspine.com
Discdegeneration Jwalant S.Mehta www.mehtaspine.com
Jwalant S.Mehta www.mehtaspine.com June2014
Facet jointchanges Jointcapsule Inferior articularprocess Superior articularprocess Increased axial rotation indisc Jwalant S.Mehta www.mehtaspine.com degeneration
Facet jointchanges Jointcapsule Inferior articularprocess Superior articularprocess Increased axial rotation in disc degeneration results in shear ofthe enthesis and direct pressure upon the capJswaulalnetS. Mehta
Facet jointchanges Inferior articularprocess Superior articular process Encompassing joint formation develops through directcontact ofenthesophytes in advanceddegeneJwraalatnitoS. nMehta www.mehtaspine.com
Facet jointchanges In contrast to other joints, reactions of the joint capsule / enthesis are seen before permanent cartilagedamage Early restoration of disc biomechanics may prevent progression to stage of permanentdamage Vernon-Roberts & Pirie RheumatolRehabil 1977 Fujiwara et al. Eur Spine J1999
Facet jointdegeneration • Jointwidth • Articularerosions • Sub-chondralsclerosis • Osteophytes Jwalant S.Mehta www.mehtaspine.com June2014
Facet jointchanges JwalantS.Mehta ww.mehtaspine.com w
Two views of a typical facet joint contact space object (for a normalspine) Volume(mm3) 309.50 SuJwralfaantcS.eMehatarea(mm2) Jun4e200144.25 www.mehtaspine.com 48
Surface area of the facet joint contact space (mean ±stdev) 1400 1200 1000 Surface area(mm2) 800 600 400 200 0 L1-2-R L1-2-L L2-3-R L2-3-L L3-4-R L3-4-L L4-5-R L4-5-L L5-S1-R L5-S1-L Jwalant S.Mehta www.mehtaspine.com
Volume of the facet joint contact space (mean ±stdev) 1400 1200 1000 Volume(mm3) 800 600 400 200 0 L1-2-R L1-2-L L2-3-R L2-3-L L3-4-R L3-4-L L4-5-R L4-5-L L5-S1-R L5-S1-L
Clinical effects of plumb-lineshifts Glassman, Bridwell et al. Spine2005 Jwalant S.Mehta www.mehtaspine.com June2014
deformity Jwalant S.Mehta www.mehtaspine.com June2014
Hyperextlat Standinglat Jwalant S.Mehta www.mehtaspine.com June2014
Aim1:achievefusion • Good pain relief; 69 – 87% • Kostuik Clin Orthop1973 Swank JBJS Am1981 • Improvement in the lumbarlordosis • Anterior column load sharing Jwalant S.Mehta www.mehtaspine.com
Aim 2: adaptation oflordosis • Excise facetjoints • ‘Open’ degenerate discspaces • LL=PI ±90 • Measure the PI, and build in thelordosis Jwalant S.Mehta www.mehtaspine.com
Adult Deformity: Surgicalgoals • Normalize & balancecontours • Fuse the least number ofsegments • Neuraldecompression • Obtain solid biologicalfusion Jwalant S.Mehta www.mehtaspine.com
Adult Deformity: principles ofsurgery • Traction + erect full spinefilms • Measureparameters • Levels toinstrument • Levels todecompress • Anterior columnmanagement Jwalant S.Mehta www.mehtaspine.com June2014
MM 86Y Jwalant S.Mehta www.mehtaspine.com June2014