Download
1 / 38
440 likes | 1.37k Views
Spinal Surgery in the Dog. Review localization of compressive lesions of the spinal cord. . Upper motor neuron lesions: Paresis or paralysis Intact = hyperreflexia Preserved = increased muscle tone Atrophy = from disuse Lower motor neuron lesions: Paresis or paralysis

E N D
Review localization of compressive lesions of the spinal cord. Upper motor neuron lesions: Paresis or paralysis Intact = hyperreflexia Preserved = increased muscle tone Atrophy = from disuse Lower motor neuron lesions: Paresis or paralysis Decreased = hyporeflexia Hypotonia = decreased muscle tone Neurogenic atrophy
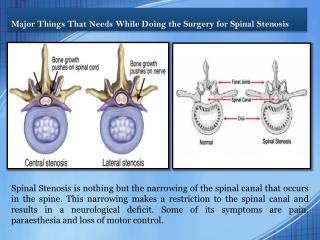
Spinal cord lesions: • If lesion is between C1-C5=UMN lesion • If lesion is between C6-T2=(area of innervation of forelimbs)= LMN lesion • If lesion is between T3-L3=UMN lesion • If lesion is between L4-S1=(area of innervation of pelvic limbs)=LMN lesion • If lesion is between S2-S3=LMN to bladder and rectal sphinters disrupted • If lesion is between Cd1-Cd5=LMN to tail muscle are disrupted
What are the important components of conservative treatment for spinal cord disease? • Used for management of mild cases and for postoperative management • Conservative treatment includes: • Absolute cage rest • Anti-inflammatory drugs +/- muscle relaxants • Serial neurological examinations
What is the most common cause of failure? • b/c owner does not provide accurate cage rest
Why is fenestration alone seldom used in management of spinal cord disease? • Because it does not remove the nuclear material from the spinal canal and foramina, only from intervertebral spaces, therefore need another procedure for the other areas
Why is it used in conjunction with decompressive surgery? • reduces risk of recurrence of disk disease
What are the 2 decompressive approaches for the cervical spinal cord? • Ventral slot decompression • Cervical dorsal laminectomy and hemilaminectomy
What approaches are used for the thoracolumbar spinal cord? • Fenestration • Dorsal laminectomy • hemilaminectomy
When is a durotomy indicated? • Used for decompression of spinal cord and for direct examination of traumitized cord to assess damage
Describe postoperative management of the spinal surgery patient. • Cage rest – water bed, air mattress • Hydrotherapy, tail walking, passive range of motion exercise • Care of urinary tract: • Empty bladder at least 3 times/day • Culture urine, treat as needed
In general, which neurological functions return first? • Normal urination = 10-21 days • Normal pain sensation = 10-21 days • Voluntary paddling motions= 14-35 days • Voluntary support of weight=14-42 days • Ambulation= 14-90 days • Proprioception= 21-180 days
What is the average time interval for recovery of urinary tract function? • 10-21 days
of complete function? • I am assuming this means complete fxn of everything…. • 21-180 days = proprioception last to return
Compare Hansen’s Type I and Hansen’s Type II Disk Disease in terms of: etiopathogenesis, signalment, history, neurological signs and presenting complaint, prognosis. • Hansen’s type I: • Etiology: • chondroid degeneration of disk • Nucleus pulposis becomes granular or calcified and thus less compressible • Annulus ruptures and nucleus is extruded into spinal canal or foramen • Signalment: • Chondrodystrophoid breeds = dachshund and beagle are most commonly affected • Adult, usually middle aged • No sex predillection • Disk rupture may occur with normal activity • HX:???? • Hansen’s Type II: • Etiololgy: • Fibrinoid metaplasia of disk – common aging change in disk • Annulus fibrosis hypertrophies and protrudes into ventral spinal canal but does not rupture • No extrusion of nuclear material • Signalment: • Non-chondrodystrophoid breeds,often large breeds • Middle age to old dogs • No sex predilection
Why is the Hansen’s Type I patient with thoracolumbar disk extrusion more likely to show severe signs of cord compression than the patient with cervical disk protrusion? • because cervical herniation has the dorsal longitudinal ligament which decreases the cord compression
What are the indications for decompression in Hansen’s Type I patients with cervical disk extrusion? • Neurological abnormalities, severe pain, frequent repeated episodes of mild pain • Rad evidence of disk material compressing the spinal cord or nerve root • Deterioration while undergoing conservative treatment
What are the indications for these patients when the disk extrusion is in the thoracolumbar region? • Recurrent pain +/- mild paresis • Severe paraparesis • Paraplegia +/- deep pain sensation • Patient that becomes worse during conservative tx
List 3 factors associated with poor prognosis for these patients. • Acute onset • Severe neuro signs • Duration of paraplegia >48 hours
What are the types of lesions seen in wobbler’s syndrome? • Type 2 disk • Vertebral tipping • Congenital osseous malformation • Hourglass compression • Ligamentum flavum/ vertebral arch malformation
Which 2 are most common? • Type 2 • Vertebral tipping
Which may be dynamic? • Chronic degenerative disk disease • Vertebral tipping • Malformation of the vertebral arch w hypertrophy of the ligamentum flavum
In what position of the neck are these animals worse? • If they hold their head up (dorsal extension)
Describe medical management for the patient with wobbler’s syndrome. When is it indicated? • Indicated for dogs with pain only or with mild weakness and motor deficits • Strict confinement for 3-4 weeks followed by gradual return to normal activity over next 3-4 weeks • Neck brace • Use of harness instead of collar • Anti-inflammatory drugs
What are the 3 objectives of surgical treatment? • Relief of SC compression • Cervical spinal stabilization • Reversal of neuro deficits
If you were to do surgery on a dog with a Type II disk lesion and ventral vertebral tipping, what approach would you choose? • Ventral
If this dog had a dynamic compressive lesion, what additional procedure (in addition to decompression) would be required? • Ventral stabilization-traction
Define cauda equina syndrome. • Complex of neuro signs caused by compression of the terminal nerve roots in the lumbosacral spinal canal
What are the common history and clinical signs? • Chronic lameness, back pain and hind limb weakness • Urinary or fecal incontinence • Abnormal tail carriage or movement • Muscle atrophy • Self mutilation of the tail or hind feet
What is the surgical approach and treatment? • Dorsal laminectomy +/- facetectomy and removal of interarcuate ligaments • Retract nerve roots to remove disk • Remove fibrous tissue surrounding nerve roots • Stabilize, if instability is diagnosed
What 1 neurological abnormality is most often associated with a poor prognosis? • Chronic cases with incontinence
Define atlanto-axial instability • An alteration of the dens or the ligaments of the atlantoaxial articulation that causes instability, vertebral subluxation and spinal cord or nerve root compression
What is one very important problem to avoid during physical examination and radiography of these patents’? • Avoid flexion of the neck and avoid open mouth views when doing rads
Describe, in general terms, 2 surgical methods of treating this condition. • Ventral approach: removal of dens and reduction of subluxation; Cross pin stabilization • Dorsal approach: hemilaminectomy place suture through dorsal process of axis and arch of axis
Where are spinal fractures most likely to occur? • C2 • L1 • L7
When will you treat these fractures conservatively? • If patient has good motor and sensory function treat conservatively
When is surgical treatment required? • If motor or sensory function is impaired decompression and stabilization are indicated
Review the types of stabilization that can be used on these fractures. • Cervical fx • Dorsal stabilization: wire or screw fixation of laminae or articular facets • Ventral stabilization: cross pins +/- bone cement, ventral plate or interbody screw fixation • Thoracolumbar fx • Hemilaminectomy • Dorsal spinous process stabilization plus body cast • Vertebral body plates • Dorsal cross pins and bone cement • Combination techniques (pins and bone cement + Lubra plate)