Download
1 / 31
400 likes | 1.69k Views
The Spleen. Lecture Conference Steven J. Binenbaum, MD SLR September 12 th , 2007. Splenectomy for Hematologic Diseases. Rarely cures the disease Alleviates symptoms Corrects hematologic abnormalities Staging & Diagnosis. Splenectomy for Hematologic Diseases.

E N D
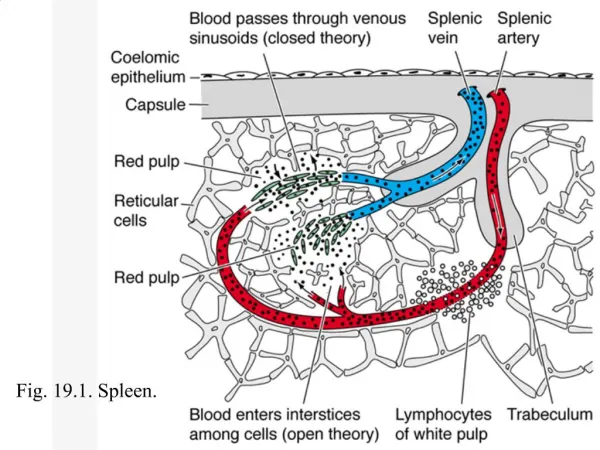
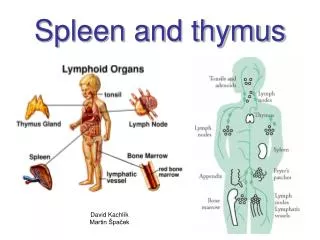
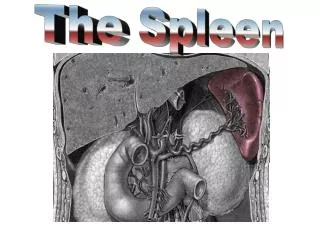
The Spleen Lecture Conference Steven J. Binenbaum, MD SLR September 12th, 2007
Splenectomy for Hematologic Diseases • Rarely cures the disease • Alleviates symptoms • Corrects hematologic abnormalities • Staging & Diagnosis
Splenectomy for Hematologic Diseases Red Cell-Related Indications Hereditary Spherocytosis (HS) • Most common type of hemolytic anemia • Autosomal dominant • Spectrin deficiency (RBC membrane) → Loss of osmotic stability • Osmotic fragility testing • Splenomegaly & Gall stones • Dx by (+) spherocytes in the blood • TOC is Splenectomy in the 4th year of life • +/- cholecystectomy if (+) cholelithiasis
Splenectomy for Hematologic Diseases Autoimmune Hemolytic Anemia (AIHA) • Warm-antibody autoimmune HA • Autoantibody opsonization and phagocytosis • Intravascular destruction or by spleen macrophages • Treatment Of Choice • #1 is Corticosteroids 1-2 mg/kg/day • PRBC’s for severe anemia • Splenectomy (80% favorable clinical response) if: • medical tx fails • Intolerance to steroids or its side-effects
Splenectomy for Hematologic Diseases Pyruvate kinase Deficiency • Autosomal-recessive disease • Splenomegaly • TOC • Splenectomy • Reduces PRBC’s requirements G6PD Deficiency • Splenomegaly is rare • Splenectomy is not indicated!
Splenectomy for Hematologic Diseases Sickle Cell Disease (SCD) • B-globin gene A→T substitution (Hb S/SS) • autosomal dominant • Sickling of RBCs in tissues with low O2 tension • Red & White pulps • Splenic microinfarcts • Painful • Abscess • Infections • Anemia • Splenectomy (palliative) • Acute sequestration crises (recurrence = 40%-50% with 20% Mortality rate) • Rapid hypersplenism • Abscess formation
Splenectomy for Hematologic Diseases Thalassemia • Thalassemia major (homozygous B) • autosomal-dominant disease • Decreased expression of beta-chains • Pallor, Growth retardation, head enlargement • Splenectomy indicated if: • Symptomatic splenomegaly • Anemia • Pain due to infarctions • increased PRBC’s requirements (>200 ml/kg/year) • ↑ rate of infections after splenectomy • Risk vs. Benefit
ITP Spleen is not enlarged ♀ > ♂; Renal insufficiency children vs. adults Self-limited in children (70%) Splenectomy is for rare cases Insidious onset in adults ↓ Plts < 10,000/mm3 #1 TOC is PO Steroids 1-1.5 mg/kg/d (up to 70% response) IVIG 1 g/kg/d x2-3 days Splenectomy if fail steroid tx TTP Splenomegaly Microvascular thrombosis Petechiae, fever, neurologic changes #1 TOC Plasmaphoresis Splenectomy is #2 Durable remission? Avoid PLT transfusions ↑ morbidity Splenectomy for Hematologic DiseasesPlatelet Related Indications
White Cell - Related Indications Leukemia • CLL & Hairy cell leukemia (HCL) • Splenectomy • improves cytopenias (75%) • Ameliorates symptomatic splenomegaly Non-Hodgkin’s Lymphoma (NHL) • Splenectomy • Painful splenomegaly • Cytopenia • No role for staging
White Cell - Related Indications Hodgkin’s Disease • Current indications for surgical staging: • Stage I or Stage II with NS histology and w/o B-symptoms • Staging procedure • Wedge liver biopsy • LN sampling: • Retroperitoneal • Mesenteric • Hepatoduodenal • Splenectomy
Bone Marrow – Related Indications • Myelofibrosis & Myeloproliferative disorders • Splenectomy for symptoms due to enlarged spleen
Splenectomy Complications • LLL atelectasis, pneumonia, effusion • Hemorrhage (mostly with laparoscopic) • Intraabdominal abscess (LUQ) • Pancreatitis or fistula formation • DVT • PVT • Hemolytic anemia or myeloproliferative dz with splenomegaly • OPSI
Splenectomy Complications OPSI • Incidence ≈1% (up to 5%); 50% Mortality • Encapsulated gram-positive bacteria = Streptococcus • Risk factors • Children < 15 yrs old • Immunosupression • Hematologic dz (thalassemia, SCD, etc) • Highest within the first 2 yrs post splenectomy • Pnemococcus, H.influenza, meningococcus • vaccination 7-14 days prior to splenectomy • Pneumovax booster Q5yrs and annual H.influenza immunizations • Abx prophylaxis for children x2 yrs post splenectomy • Lower incidence of OPSI in adults (vs children) and after trauma
Tumors, Cysts, and Abscesses of the Spleen Steven J. Binenbaum, MD September 12th, 2007 SLR
Malignant Tumors • Spleen - mostly secondary involvement • non-Hodgkin’s Lymphoma – most common malignancy • Main Tx: Chemo +/- RT • Spleen is the primary site • 10% Hodgkin’s disease • 30% of resected spleens (staging procedure) have (+) histology • Hairy cell leukemia • Resect for symptomatic splenomegaly • Improved survival • CML & CLL • symptomatic splenomegaly = splenectomy
Malignant Tumors • Angiosarcoma • Nonlymphoid malignant tumor of the spleen • Early metastatic disease • Aggressive with rapid growth • Spontaneous splenic rupture and hemolytic anemia • Palliation Benign Tumors • Hemangioma • Risk of rupture + platelet sequestration (Syndrome?) • No tx unless symptomatic • Hamartoma • Lymphangioma
Nonparasitic Epithelium-lined cysts Epidermoid cysts – most common Mostly asymptomatic Young children + young adults LUQ pain, N/V, early satiety Dx: CTscan (+)unilocular +/- Ca++ Complications Infection, bleeding, rupture Tx: Splenectomy partial Parasitic 5% in US Abroad – Hydatid disease Echinococcus granulosus Mostly asymptomatic Associated with liver cysts If only spleen is involved? Tx: Splenectomy Splenic Cysts
Splenic Cysts • Splenic Pseudocysts • Lack epithelial lining • Account for most cystic splenic dz in US • Pancreatic pseudocyst • Posttraumatic • Splenectomy is indicated when: • Size >10 cm or • symptomatic
Splenic Abscess • Uncommon, but fatal • Erode into adjacent structures • Most are secondary in etiology • Bacterial endocarditis • Intrabdominal infections (pyelo-, etc) • IVDA • Infected splenic hematoma • Infected splenic infarctions (embolizations, ischemia, etc) • S/S: fever, WBC; • 50% (+) blood cultures • Dx by CT scan + IV contrast • Staphylococcus & Streptococcus • E.coli, Salmonella, anaerobes • Tx: • Splenectomy + IV Abx • Percutaneous drainage
Splenic Salvage Procedures: Therapeutic Options SLR September 12th, 2007
Nonoperative Management of Splenic Trauma Indications for initial nonoperative management • hemodynamic stability • absence of peritonitis • CT scan • No contrast extravasation • absence of other injuries • Transfusions - >2 PRBC’s
Protocol for Nonoperative Management Grade I & II • Awake + alert, isolated injury • monitored observation • BR, H/H q6h, serial abdominal exams • Regular floor in 48º • If remain stable and asymptomatic – D/C in 5 days • F/U CT scan in 4 wks • Avoid prophylactic and therapeutic heparinization • Grade III, IV, & V • Monitored observation x5 days • Repeat CT scan • Transfer to floor if stable • F/U CT scan in 6-8 wks after discharge
Splenorrhaphy • Topical Hemostasis • Small injuries (I & II) • Bovie electrocautery • Argon beam • Gelfoam • Surgicel • Avitene • Suture Repair & Partial Resection • Segmental blood supply • Monofilament sutures • Pledgeted horizontal mattress sutures
Splenorrhaphy • Mesh Splenorrhaphy • Delaney (1982) • Autotransplantation • controversial