Download
1 / 27
270 likes | 562 Views
IDIOPATHIC MESENTERIC PANNICULITIS. M. LIMEME, H. ZAGHOUANI BEN ALAYA, H. AMARA, D. BEKIR, CH. KRAIEM Imaging department, Farhat Hached Hospital, Sousse, Tunisia. GI26. Introduction. Synonyms: retractile mesenteritis, fibrosing mesenteritis,

E N D
IDIOPATHIC MESENTERIC PANNICULITIS M. LIMEME, H. ZAGHOUANI BEN ALAYA, H. AMARA, D. BEKIR, CH. KRAIEM Imaging department, Farhat Hached Hospital, Sousse, Tunisia GI26
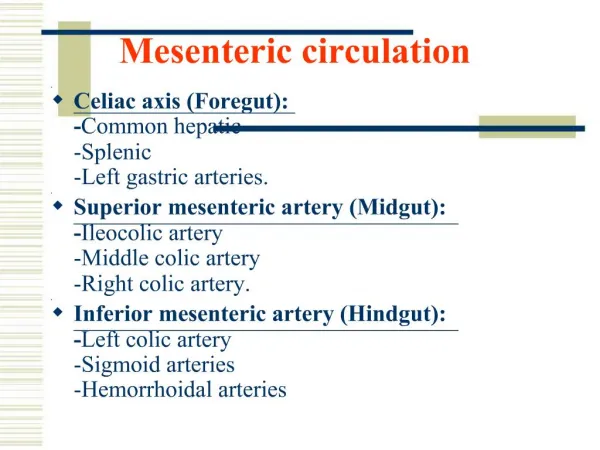
Introduction • Synonyms: retractile mesenteritis, fibrosing mesenteritis, mesenteric panniculitis, mesenteric lipodystrophy, liposclerotic mesenteritis, systemic nodular panniculitis. • Definitions: Complex mesenteric inflammatory disorder of unknown etiology
Objectives To describe the imaging features of non-specific inflammation of mesenteric fat tissue without associated pathology and to formulate differential diagnosis.
Materials and Methods • Among two men and a women (mean age 45 years), 2 were paifull, • Diarrhea was noted in two cases, • And fever in one case. • An abdominal mass was found in two cases, • 3 patients had an inflammatory syndrome.
Results • The diagnosis was suggested by computed tomography (CT): (single mass: 2 cases, diffuse mesenteric thickening: 1 case) and confirmed by pathology. • Two patients were treated with corticosteroids. During the follow-up (mean 56 months) the panniculitis was stable on CT in 2 cases and regressed in one case. • No associated pathology has emerged.
Abdominal pain and diarrhea CT findings: fat ring sign (arrowheads) and tumoral pseudocapsule (arrow).
Abdominal pain and diarrhea CT findings: Solid soft tissu mass in the root of small bowel mesentery ecasing mesenteric vessels.
Abdominal mass and fever CT findings: extensive infiltration of small bowel mesentery ecasing mesenteric vessels.
Clinical issues • Symptoms: Abdominal pain, fever, nausea, vomiting, weight loss, diarrhea. Palpable mass. Incidental finding in an asymptomatic patient.
CT findings Findings vary depending on predominant tissue • Area of subtle increesed attenuation in mesentery (inflamed fat): solitary/multiple; well/ill defined • Calcification, enlarged mesenteric lymph nodes, • Fatty necrotic cystic mass may be seen, • Infiltration of pancreas or portahepatis, • Encasement of mesenteric vessels and collateral vessels: narrowing/occlusion on contrast study
Increesed attenuation in mesentery (red arrow) with well defined outlines: pseudocapsule. Encasement of mesenteric vessels and collateral vessels (blue arrow)
CT findings • « Fat ring » sign: preservation of fat arround vessels: • Hypodense fatty halo surrounding mesenteric vessels and nodules, • Predominantly seen in mesenteric panniculitis, • Differentiates scleroing mesenteritis from other mesenteric processes (lymphoma, carcinoid tumor, carcinomatosis)
« Fat ring » sign: preservation of fat arround vessels Horton and al. Radiographics. 2003 ;23(6):1561-7
CT findings • Pseudocapsule: peripheral band of soft tissue attenuation that limits normal mesentery from inflammatory process: • Seen in mesenteric panniculitis phase, • Enhancement of pseudocapsule may be seen. • Thickening/infiltration/displacement/narrowing of bowel loops.
Pseudocapsule: peripheral band of soft tissue attenuation that limits normal mesentery from inflammatory process
CT findings • « Misty mesentery »: nonspecific sign • Increesed attenuation of mesentery, • Evidence of small mesenteric nodes, • No discret soft tissu mass, • Seen in any pathology that infiltrates mesentery
CT findings • Solid soft tissu mass usually in root of small bowel mesentery (fibroous tissue) • Single/large/lobulated/ill-defined increesed density mass with linear radiating strands (fibroma-rare) • Small mesenteric soft tissue nodules of increesed density (fibromatosis)
MRI findings • Variable signal intensity due to: inflammation, fat, fibrosis, vascular and Ca++. • Mesenteric panniculitis and lipodystrophy: • T1WI: mixed signal intensity, • T2WI: mixed signal intensity. • Retractile mesenteritis: in mature fibrotic reaction • T1WI: decreesed signal intensity, • T2WI: very low signal intensity, • Gradient-écho MR image: *Narrowing/occlusion of flow in mesenteric vessels *Collateral vessels are seen
Differential diagnosis • Non-Hodgkin lymphoma, • Carcinoid tumor, • Mesenteric edema, • Desmoid tumor (Fibromatosis), • Carcinomatosis (mesenteric metastasis)
Differential diagnosis Non-Hodgkin lymphoma
Differential diagnosis Carcinoid tumor
Differential diagnosis Mesenteric edema
Differential diagnosis Desmoid tumor
Differential diagnosis Carcinomatosis (mesenteric metastasis)
Treatment • Steroids, colchicine, immunosuppressive agents: before fibrotic changes. • Surgical excision: fibrosis and retraction with obstructive symptoms.
Conclusion • Various diseases (usually malignant) can mimic the imaging features or be associated. • Pathological verification leads to affirm the idiopathic mesenteric panniculitis, a benign entity of unknown pathogenesis. • Corticosteroid therapy is reserved for symptomatic patients.