Download
1 / 31
330 likes | 1.18k Views
Omental and Mesenteric Conditions. Omentum. I. Anatomy - double sheet of flattened endothelium - epiploic vessels, lymphatics, nerves, and fatty areolar tissue pass in between

E N D
Omentum I. Anatomy - double sheet of flattened endothelium - epiploic vessels, lymphatics, nerves, and fatty areolar tissue pass in between - hangs as a double fold between the greater curve of the stomach to the transverse colon, with the right side usually longer and larger
- size depends on the amount of fat - usually underdeveloped in innfants II. Physiology - “Policeman of the abdomen”; helps in walling of inflammatory conditions - areolar tissue is rich in inflammatory conditions
III. Pathology A. Torsion – twisting along its long axis causing vascular compromise * requirements for torsion - redundant segment - a fixed point
1. Etiology a. Primary - with predisposing factors such as projections from the edge of the omentum, obesity, and venous redundancy
b. secondary - associated with another pathology such as omental cysts, tumors, inflammatory conditions or hernias 2. Pathology a. twists in a clockwise direction b. right side twists more frequently
3. Clinical manifestations a. pain - sudden, constant, increasing in intensity b. nausea and vomiting c. peritonitis d. mass
4. Diagnosis - laparotomy 5. Treatment - resection B. Idiopathic Segmental Infarction – acute vascular occlusion not accompanid by torsion, intraabdominal conditions, trauma, or cardiac disease 1. Etiology – thrombosis of the omental veins secondary to endothelia injury
- usually involves the right side 2. Clinical manifestions – pain which is gradual in onset, usually on the right side 3. Diagnosis – CT scan which will show a “smudged” appearance
4. Treatment – excision C. Cysts 1. Pathology a. obstructed lymphatic channels b. growth of congenitally misplaced lymphatic tissue
2. Clinical manifestations – palpable mass 3. Diagnosis a. x- ray – can diagnose dermoid cyst b. ultrasound c. CT scan
4. Treatment – excision D. Solid tumors 1. Pathology a. metastatic carcinoma – most common b. hemangiopericytoma and leiomyosarcoma – most common primary tumors
2. Diagnosis a. ultrasound b. CT scan 3. Treatment – excision of the primary tumor if possible and omentum
Mesentery I. Anatomy - a reflection of the posterior peritoneum - connects the intestines to the posterior abdominal wall and carries blood vessel and nerves - root of the mesentery extends from the ligament of Treitz at the level of L2 and is approximately 6 inches
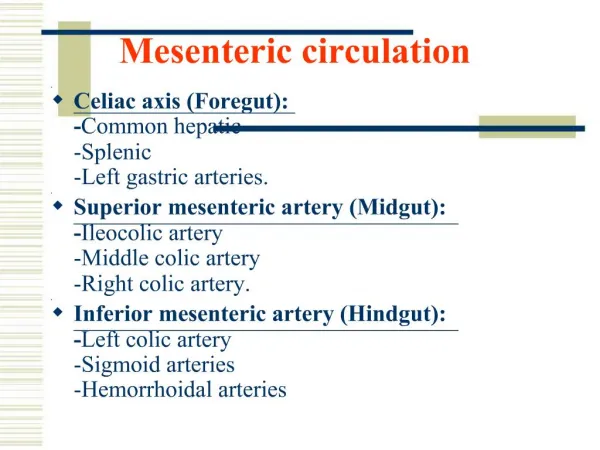
- Mesocolon – suspensory ligament of the transverse and sigmoid colon - Space of Riolan – avascular space to the left of the middle colic artery - Mesenteric circulation
B. Pathology 1. Acute Occlusion of the SMA a. embolism - sudden occlusion of the main branch of the SMA - produces ischemia of the entire small bowel distal to the ligament of Treitz and proximal half of the colon
b. thrombosis - occurs in an artery partially occluded by atherosclerosis - slowly developing stenosis may allow time for collaterals to develop
2. Pathology - sudden complete occlusion first causing an ischemic infarct in which the bowel is pale - later stages will show hemorrhagic infarction
3. Clinical Manifestations - surgical emergency with extreme abdominal pain - P.E. is not proportional to the pain the patient perceives - unresponsive to narcotics - mottled, cyanotic abdomen - absent bowel sounds
4. Diagnosis a. arteriogram b. WBC – leukocytosis c. hct – hemoconcentration d. metabolic acidosis e. FPA – dilated bowel loops
5. Treatment a. embolectomy b. resection c. antibiotics d. anticoagulation e. NGT
B. Non- occlusive Mesenteric Infarction 1. Etiology – low cardiac output from CHF, MI, septic shock, arrythmia 2. Diagnosis – arteriography 3. Treatment a. correct hypotension b. vasodilators c. antibiotics
C. Chronic Occlusion of Visceral Arteries 1. Etiology – “intestinal angina” - ischemia without infarction - food pain sequence 2. Pathology – occlusion secondary to atherosclerosis
3. Clinical Manifestation – crampy abdominal pain when eating with weight loss 4. Diagnosis – arteriogram
5. Treatment a. arterial reconstruction b. thromboendarterectomy c. synthetic vein graft d. resection
D. Occlusion of Mesenteric Veins 1. Etiology – usually secondary to thrombosis 2. Pathology – hyperemia, edema, subserosal hemorrhage 3. Clinical Manifestations – vague discomfort, severe abdominal pain 4. Treatment – resection, antibiotics, anticoagulant