Download
1 / 72
720 likes | 1.06k Views
The 17th Conference on Retroviruses and Opportunistic Infections. San Francisco, CA February 16-19, 2010. Studies in ARV-Naïve Patients When to Start. Rick Elion, MD Associate Professor, George Washington University School of Medicine Washington, DC.

E N D
The 17th Conference on Retroviruses and Opportunistic Infections San Francisco, CA February 16-19, 2010
Studies in ARV-Naïve PatientsWhen to Start Rick Elion, MD Associate Professor, George Washington University School of Medicine Washington, DC
Life Expectancy ofHIV-Positive Patients Years of Life Remaining Years of Life Remaining Age at time of death Years lived Remaining Life Years Age at 24 weeks (years) General Population Asymptomatic HIV+ Patients Comparison of life expectancy of Athena cohort patients to general population (n=4174) Age at week 24, country of birth and stage B symptoms were associated with a higher risk of death Expected life years remaining at age 25 was 53.1 (44.9-59.5) for general population and 52.7 for asymptomatic HIV+ patients The modeled life expectancy of patient presenting at an older age and women were slightly lower that general population van Sighem A, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 526.
Increasing CD4 at First Presentation but Patients Still Present Late to Care NA-ACCORD analysis regarding median CD4 on first presentation from 1996-2007 (N=35,009) Median CD4 on presentation has increased from 234 to 327 cells/mm3 (P<0.01) Proportion of CD4 ≥350 cells/mm3 at first presentation has increased from 34% to 47% (P≤0.01) Althoff K, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 982.
Linkage of Testing to Routine Care Leads to Earlier Diagnoses p<0.001 Washington DC has an estimated HIV seroprevalence of 3% 2006 DOH expanded HIV testing to be included in routine care with improved clinical linkages From 2004 to 2006, HIV tests increased from 19,000 to 73,000 Among newly diagnosed, median CD4 count increased 57% Castel A, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 34.
CD4 at Initiation of ARV Therapy Predicts Extent of CD4 Recovery Median CD4+ cell count 1,378 patients at 10 US clinics followed from 1996-2007 Median Peak CD4 was progressively higher for specific CD4 strata (p<0.001) Multivariate analysis: Increased mortality with CD4 < 50 (HR=4.6) and CD4 50-199 (HR=2.6) compared to ≥200 cells/mm3 Lower BL CD4 at initiation also associated with increased risk of death from non-AIDS-related causes. Palella F, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 983.
Correlation Between Nadir CD4+ T-cell Count and Cardiovascular Risk • Cross-sectional study of 80 HIV+ men on ARV Tx with undetectable HIV RNA • Median age 47 years, nadir CD4+T cell count 180 cells/mm3 • CV risk assessed using arterial stiffness (AS) by pulse wave analysis and carotid-femoral pulse wave velocity (PWV) • Nadir CD4 count <350 cell/mm3 independently associated with significant increase in AS and PWV • Other significant determinants of PWV in multivariate analysis included age, systolic and diastolic BP, and diabetes. • AS was not affected by the duration of ARV therapy or exposure to PIs or ABC. Significant determinants of PWV on Multivariate Analysis Ho J, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 707.
Neurocognitive Disorders Associated with Nadir CD4 Counts Odds Ratio for Cognitive Impairment by CD4 Nadir 1.1 1 0.9 0.8 0.7 0.6 0.5 0.4 0.3 Odds Ratio <50 50-199 200-349 ≥350 CD4 Nadir Odds Ratios for NP Impairment • Multicenter cohort study (CHARTER) of 1526 pts evaluating HIV-associated Neurocognitive Disorders (HAND) • Complex testing consistent with defined criteria used to determine HAND • 603 had HAND (without a substantial confounder); 726 not impaired • Most with HAND (n=428) were asymptomatic and only a few (n=27) had frank dementia • Multivariate analysis: Higher CD4 nadir associated with lower risk of HAND Ellis R, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 429.
Impact of Expanded HAART Availability on New HIV Diagnoses New HIV + Diagnoses (All) Active on HAART New HIV + Diagnoses (IDU) Evaluation of association between expansion of ART coverage, population level HIV viral load and new HIV diagnoses in British Columbia Expansion of ART access in 2004-2009 associated with a significant decline in new HIV diagnoses After 2007, ~50% decrease in new HIV diagnoses among IDU occurred and associated with a decline in proportion of HIV+ IDU with plasma HIV-1-RNA level >1500 copies/mL from ~50% (2000-2004) to ~20% (2009) (P<0.001) Montaner J, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 88LB.
Studies in ARV-Naïve PatientsWhat to Start Joseph Eron, MD Professor, University of North Carolina School of Medicine Chapel Hill, NC
Elvitegravir and Cobicistat (GS-9350):Design of the Two Phase 2 Studies EVG/GS-9350/TDF/FTC + placebo n=48 Treatment-naïve HIV RNA ≥5,000 copies/mL CD4 cells >50 cells/mm3 No Resistance to NRTIs NNRTIs PIs HBV- and HCV-negative 2:1 EFV/TDF/FTC + placebo n=23 GS-9350 + placebo ATV + FTC/TDF n=50 2:1 RTV + placebo ATV + FTC/TDF n=29 • Randomization stratified by HIV RNA (≤ or >100,000 copies/mL) • Primary Endpoint: Proportions with HIV RNA <50 copies/mL at Week 24 • 48-week trials Cohen C, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 58LB.
Baseline Characteristics Cohen C, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 58LB.
Primary Endpoint: Percentage with HIV RNA <50 copies/mL (ITT M=F) RTV vs. GS-9350 EVG/GS-9350 vs. EFV Week 24 stratum-weighted difference -1.9% (95% CI: -18.4% to 14.7%) Week 24 stratum-weighted difference +5% (95% CI: -11.0% to 21.1%) 100 100 90% 86% 83% 80 84% 80 60 60 HIV RNA <50 copies/mL Percentage with Percentage with HIV RNA <50 copies/mL 40 40 20 20 0 0 0 4 8 12 16 20 24 0 4 8 12 16 20 24 Week Week RTV + ATV + TDF/FTC EVG/GS-9350/TDF/FTC GS-9350 + ATV + TDF/FTC EFV/FTC/TDF Cohen C, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 58LB.
Adverse Events >5% Related to Randomized Drug Cohen C, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 58LB.
A5202: Study Design HIV-1 RNA ≥1000 c/mL Any CD4+ count ≥16 years of age Stratified by screening HIV-1 RNA (< or ≥100,000 c/mL) EFV QD TDF/FTC QD TDF/FTC QD ABC/3TC Placebo QD ABC/3TC Placebo QD EFV QD ABC/3TC QD ABC/3TC QD HIV+, ART-naïve(N=1857) TDF/FTC Placebo QD TDF/FTC Placebo QD ATV/r QD ATV/r QD Daar E, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 59LB.
A5202: Overall Baseline Characteristics * Required for those with recent infection, otherwise optional Daar E, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 59LB.
A5202: Time to Virologic Failure in Patients with Baseline HIV RNA >100,000 c/mL TDF-FTC (26 events) ABC-3TC (57 events) P<0.001, log-rank testHazard ratio, 2.33 (95% CI, 1.46-3.72) Probability of No Virologic Failure Results similar between EFV and ATV/r arms Sax PE, et al. NEJM 2009;361:2230-2240; Daar E, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 59LB.
Probability of No Virologic Failure and CD4+ Change at Week 96 All Subjects HIV RNA <100,000 c/mL Percent without Virologic Failure Percent without Virologic Failure HR 1.13 (0.82,1.56) HR 1.26 (0.76,2.05) HR 1.23 (0.77,1.96) HR 1.01 (0.70,1.46) ABC/3TC TDF/FTC EFV ATV/r 250 251 252 221 CD4 Change (cells/mm3) P= 0.89 0.002 Daar E, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 59LB.
A5202: Percent of Virologic Failures with Emergence of Major Resistance Mutations ABC/3TC TDF/FTC Viral failures No baseline resistance (N) 48 76 54 63 P<0.0001 P<0.0001 Percent P=0.0003 P=0.046 P-values: ATV/r vs. EFV (among failures) *Major mutations defined by IAS-USA (2008) list plus T69D, L74I, G190C/E/Q/T/V for RT and L24I, F53L, I54V/A/T/S and G73C/S/T/A for PR Daar E, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 59LB.
ACTG 5208: Study DesignOctane Trial II Only African sites; partner study to same comparison in women who had received sdNVP LPV/r + TDF/FTC ART-naïve women with CD4+ <200 cells/mm3 (N=500) NVP + TDF/FTC Open-label comparison of NVP and LPV/r, both combined with TDF/FTC Median F/U (weeks) 120 • Two primary endpoints: • Time to VF/death • Time to discontinuation 116 Boltz V, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 154.
OCTANE 1: Results Among Women with Prior sdNVP Exposure Virologic Failure or Death Adjusted HR 3.6 (95% CI: 1.7-7.5) Patient Percent NVP LPV/r sdNVP=Single-dose NVP Boltz V, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 154.
ACTG 5208/OCTANE 2:Results at 168 Weeks Discontinuation Virologic Failure or Death HR 3.4 (95% CI: 2.2-5.5) HR 0.85 (95% CI: 0.56-1.29) LPV/r NVP Patient Percent Patient Percent • VF: LPV/r 17% vs. NVP 15% • Death: LPV/r 3% vs. NVP 2% • Pts D/C due to AE: NVP 35 vs. LPV/r 0 • Hepatic events 20, rash 12, hepatic/rash 2 Boltz V, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 154.
Studies in Treatment-Experienced Patients And Investigational Compounds Calvin Cohen, MD Research Director, CRI New England Harvard Vanguard Medical Associates Boston MA
ODIN: Study Design Treatment phase (up to 48 weeks) • ARV-experienced patients, aged 18 years • HIV-1 RNA >1000 copies/mL • CD4 cell count >50 cells/mm3 • No DRV RAMs at screening* • Stable HAART for 12 weeks DRV/r 800/100mg qd + OBT‡ (n=294) DRV/r 600/100mg bid + OBT‡ (n=296) stratified by screening HIV-1 RNA (50,000, >50,000 copies/mL) * DRV RAMs include the following mutations: V11I, V32I, L33F, I47V, I50V, I54L, I54M, T74P, L76V, I84V, L89V ‡ Individualized OBT included ≥2 N(t)RTIs based on ARV history and resistance testing Only restrictions on previous therapy: use of enfuvirtide, tipranavir, DRV, current use of investigational drugs ARV = antiretroviral; HAART = highly-active antiretroviral therapy; OBT = optimized background therapy;qd = once-daily; bid = twice-daily; RAMs = resistance-associated mutations Cahn P, et al. 17th CROI; San Francisco, CA, US; February 16-19, 2010. Abst. 57 Phase IIIb, randomized, open-label study
ODIN: Key Features of Population including Prior and Concurrent ARVs ‡Using Antivirogram® Cahn P, et al. 17th CROI; San Francisco, CA, US; February 16-19, 2010. Abst. 57
ODIN: Virologic Response Rates and Resistance Outcomes Resistance Summary DRV/r 800/100mg qd DRV/r 600/100mg bid Meets Noninferiority Difference in response qd vs. bid (ITT): 72.1–70.9 = 1.2% (95% CI = –6.1%, 8.5%) 100 Response by Screening HIV RNA 80 78.4% 60 76.8% % HIV-1 RNA <50 copies/mL (% [95% CI]) 40 52.8% 52.8% 20 0 222 N= 224 72 72 >50,000 50,000 Screening HIV-1 RNA (copies/mL) ‡ Not significant; §Also DRV RAMs Cahn P, et al. 17th CROI; San Francisco, CA, US; February 16-19, 2010. Abst. 57 DRV/r 600/100mg BID DRV/r 800/100mg QD
ODIN: Summary of Safety and Lab Findings * Includes deaths (2 in qd group; 6 in bid group; none considered by investigator as related to DRV treatment Cahn P, et al. 17th CROI; San Francisco, CA, US; February 16-19, 2010. Abst. 57
VICTOR E3 & 4: DESIGN Randomized 2:1 to VCV:Placebo Treatment-experienced R5-HIV only(N=721)* Vicriviroc 30 mg + OBT (n=486) Placebo + OBT (n=235) *857 were enrolled but 721 R5 by Trofile ES; this is the MITT population and this subset was analyzed prior to any unblinding of results Week 24 Interim analysis Week 48 Final analysis 2 randomized, identical, placebo-controlled, double-blind, phase 3 trials Documented resistance to ≥2 available drug classes (NRTI, NNRTI, or PI) or ART experience of at least 6 months Primary endpoint: % HIV RNA <50 copies/mL at 48 weeks Gathe J, et al. 17th CROI; San Francisco, CA, US; February 16-19, 2010. Abst. 54LB
VICTOR E3 & 4: Pooled Efficacy Control VCV 100% 80% 60% Response by Overall Sensitivity Score 40% 70% 65% 61% 55% 20% % HIV RNA <50 c/mL 0% n=176 n=85 n=293 n=145 ≥3 ≤2 No. of Active Drugs in Background Note: Subset with 0-1 active Drug: 47% VCV (n=19) vs. 12% (n=8) on Pbo responded Gathe J, et al. 17th CROI; San Francisco, CA, US; February 16-19, 2010. Abst. 54LB
VICTOR E3 & 4: Virologic Failure, Resistance and Discontinuations Gathe J, et al. 17th CROI; San Francisco, CA, US; February 16-19, 2010. Abst. 54LB
Victor E3 & 4:Key Adverse Events *Causes of Death (1 each): Intestinal obstruction & septicemia S/P prior abdominal surgery, Homicide; Myocardial infarction (recurrent while in OR for CABG); Chronic congestive heart failure with pericardial effusion; Acute cholecystitis with septicemia; Plasmablastic lymphoma; Multiorgan system failure accompanied by cholecystitis and pleural effusion Gathe J, et al. 17th CROI; San Francisco, CA, US; February 16-19, 2010. Abst. 54LB
TBR-652: Characteristics and Potential for CCR2 Inhibition • Potent Oral CCR5 and CCR2 receptor antagonist • In vitro protein-adjusted EC50=0.29 nM for R5 • Neither a CYP inducer nor inhibitor • Additive / synergistic activity with other ART classes in vitro • Oral bioavailability (current formulation) enhanced by food • Once daily dosing (Plasma T ½=35-40 hours) • Study Design: Ten day monotherapy, R5-tropic pts • CCR2 receptors are associated with, and currently being studied in several inflammation-associated diseases (atherosclerosis, rheumatoid arthritis, insulin resistance) • Thus far no significant safety signals are identified with CCR2 antagonists Cohen C, et al. 17th CROI; San Francisco CA USA; February 16-19, 2010. Abst. 53
TBR-652: Median and Nadir Antiviral Response with Ten Days Monotherapy Median VL Response Nadir Viral load Response 10 day dosing Note: CCR2 inhibition observed using MCP-1 level increases Cohen C, et al. 17th CROI; San Francisco CA USA; February 16-19, 2010. Abst. 53
TBR-652: Summary of Adverse Events * AEs in 2 patients or more per cohort judged at least possibly related to study drug. Cohen C, et al. 17th CROI; San Francisco CA USA; February 16-19, 2010. Abst. 53
Studies in Resistance Issues Andrew Zolopa, MD Associate Professor, Stanford University School of Medicine Palo Alto, CA
Octane 1: Low Level NNRTI Resistant Variants Explain Virologic Failures 26% P=0.006 P=0.001 P=0.038 19% 13% 8% 9% 6% (n=120) (n=119) (n=15) (n=18) (n=105) (n=101) ASP=Allele specific PCR • Women prior SD NVP • For MTCT prevention • Randomized clinical trial: NVP vs. LPV/r • TDF/FTC backbone • NVP: Higher rate of VF (HR 3.5) • Only 1/3 of NVP failures had resistance by standard GT • Analyzed results by ASP • Frequency of >0.8% associated with increased risk of VF Boltz V, et al. 17th CROI; San Francisco CA USA; February 16-19, 2010. Abst. 154.
OCTANE 1: Virologic Outcomes by Resistance at baseline by Allele Specific PCR (ASP*) % Virologic Failure Overall Baseline GT: no NNRTI R *ASP detects specific mutations; sensitivity to 0.1% Boltz V, et al. 17th CROI; San Francisco CA USA; February 16-19, 2010. Abst. 154.
Transmitted Drug Resistance in US: Newly Diagnosed Seattle-King County HIV TDR (2007) 50% K103N Percent with TDR • 2007 CDC surveillance for transmitted drug resistance (TDR) • 10,496 with new HIV Dx • 2,480 with genotype • TDR detected in 16% of patients with new HIV diagnosis • Most common: NNRTI • 83% had single mutation • No demographic risks factors identified HIV TDR Surveillance Areas (2007) Kim D, et al. 17th CROI; San Francisco CA USA; February 16-19, 2010. Abst. 580.
Superinfection Leads to Viral Load Increases • Report of HIV superinfection in MSM (M1 and M2) • Source patient (M2) • MDR HIV on partially suppressive LPV/r + ABC/3TC regimen • Superinfected patient (M1) • HIV RNA <50 c/mL on ABC/AZT/3TC • Sudden increase in HIV RNA to >200 c/mL with further rebound • Rebound associated with 3 class resistance that matched M1 • Phylogenetically related viruses found in M1 and M2 • M1 HIV displaced by M2 HIV Castro E, et al. 17th CROI; San Francisco CA USA; February 16-19, 2010. Abst. 480.
BENCHMRK: Trial Design and Week 156 Results 200 150 100 50 0 24 48* 96* 156* Primary endpoints: Week 16 Current Analysis: Week 156 Week 240 RAL 400mg BID + OBT P018 (n=234) P019 (n=232) RAL 400mg BID + OBT HIV-1-infected Triple-class resistant HIV-1 RNA>1000 copies/mL; No CD4 cell cut-off 2:1 Placebo+ OBT P018 (n=118) P019 (n=119) RAL 400mg BID + OBT Percent of Patients (95% CI) with HIV RNA<50 Copies/mL (NC=F Approach) Change from Baseline in CD4 Cell Count(cells/mm3) (OF Approach) 164 100 80 124 62% 109 57% 50% 60 Change from BaselineCD4 Cell Count (cells/mm3) Percent of Patients with HIV RNA <50 Copies/mL 40 63 33% 20 26% 22% 45 49 0 0 0 24 48* 96* 156* Weeks Weeks Number of Contributing Patients Number of Contributing Patients Raltegravir + OBT Placebo + OBT 462 237 461 237 459 237 460 237 462 237 Raltegravir + OBT Placebo + OBT 462 237 435 230 439 228 418 219 397 208 Eron J, et al. 17th CROI; San Francisco CA USA; February 16-19, 2010. Abst. 515.
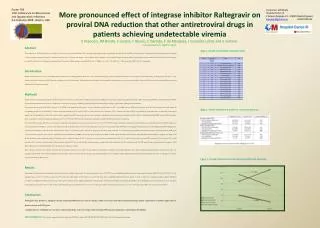
BENCHMRK: Analysis by Early HIV RNA Response in RAL Treatment Group 100% 87% Patients with low levelviremia demonstrated: – Favorable wk 156 virologic and immunologic outcomes (CD4 increase from BL +226 cells/mm3) – Significantly shorter time to loss of virologic response (TLOVR ≥400 cp/mL) compared to CS group 71% 71% 28% 17% *For HIV RNA, only discontinuations due to lack of efficacy counted as failures Eron J, et al. 17th CROI; San Francisco CA USA; February 16-19, 2010. Abst. 515.
Toxicities in Clinical Trials Paul Sax, MD Associate Professor, Harvard Medical School Boston, MA
A5202: ATV/r vs. EFVMedian Change in Fasting Lipids (Week 48) • In low HIV RNA stratum, in comparison between ABC/3TC vs. TDF/FTC: significantly greater increase in TC, LDL, HDL with both EFV and ATV/r; greater increase in TG with ATV/r Daar E, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 59LB.
A5202: ATV/r vs. EFV Median Change in Creatinine Clearance Daar E, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 59LB.
A5202: Pre-Specified Clinical Adverse Events *Defined as coronary artery disease, infarct, ischemia, angina, cerebrovascular accident, transient ischemic attack or peripheral vascular disease. Daar E, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 59LB.
A5224s: Metabolic Sub-Study of A5202 Enrolled in Substudy EFV vs. ATV/r TDF/FTC vs. ABC/3TC EFV QD TDF/FTC QD TDF/FTC QD N=69 ABC/3TC Placebo QD ABC/3TC Placebo QD EFV N=139 TDF/FTC N=139 EFV QD ABC/3TC QD ABC/3TC QD N=70 TDF/FTC Placebo QD TDF/FTC Placebo QD N=65 ABC/3TC N=135 ATV/r QD ATV/r N=130 N=65 ATV/r QD Primary endpoints (TDF/FTC vs. ABC/3TC): 1) Percent change in hip and lumbar spine BMD 2) ≥ 10% loss of limb fat Secondary endpoints: 1) bone and fat loss between EFV and ATV/r 2) on-study fractures • Study Evaluations: • DXA at 0, 24, 48, 96 weeks, then yearly • CT abdomen at 0 and 96 weeks • Serum lipids and plasma McComsey, G, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 106LB.
A5224s: Mean % Change in Lumbar Spine BMD P=0.035 P=0.004 * linear regression No significant interaction of NRTI and NNRTI/PI components (P=0.63) McComsey G, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 106LB.
A5224s: Limb Fat Changes • No statistically significant differences incidence of 10% and ≥ 20% loss of limb fat between NRTI components and NNRTI/PI components • Most study subjects gained limb fat; ATV/r increased limb/trunk fat more than EFV McComsey G, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 106LB.
STEAL: Switch to ABC/3TC or TDF/FTC Primary Results: Similar virologic results Increased risk of CV events in ABC/3TC group (8 ABC/3TC vs 1 TDF/FTC, p=0.048) not explained by lipid changes No difference in renal outcomes Loss of bone density in TDF/FTC vs gain in ABC/3TC group Inflammatory Marker Substudy 14 biomarkers (inflammatory/renal, thrombotic, endothelial function) measured at weeks 0, 12, 24, and 48 Primary analysis (change from week 0-12): No significant association between use of ABC/3TC and change in markers Alternative explanation for ABC/3TC association with CVD needed HIV+ Suppressed on 2 NRTI + PI or NNRTI (N=357) TDF/FTC FDC n=179 ABC/3TC FDC n=178 Martin Clin Infect Dis. 2009 Nov 15;49(10):1591-601; Humphries A, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 718.
Abacavir and CVD: Search for a Mechanism Increased platelet reactivity1 Carbovir TP (ABC metabolite) inhibits soluble guanylyl cyclase, a known inhibitor of platelet function increases platelet activation In vitro, ABC induces human leukocyte-endothelial cell interaction at clinically-relevant doses2 Abacavir Control 1. Baum P, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 717; 2. de Pablo C, et al. ibid., 716.