Download
1 / 17
170 likes | 306 Views
The Effect of Pravastatin on Coronary Events after Myocardial Infarction in Patients with Average Cholesterol Levels.

E N D
The Effect of Pravastatin on Coronary Events after Myocardial Infarction in Patients with Average Cholesterol Levels Frank M. Sacks, M.D., Marc A. Pfeffer, M.D., Ph.D., Lemuel A. Moye, M.D., Ph.D., Jean L. Rouleau, M.D., J. Malcolm O. Arnold, M.D., Chuan-Chuan Wun, Ph.D., Barry Davis, M.D., Ph.D., Eugene Braunwald, M.D., for the Cholesterol and Recurrent Events Trial Investigators N Engl J Med 1996; 335:1001-9
CARE - Study Design • Secondary prevention of CHD • 80 centers in the US and Canada • 4159 men and women aged 21 to 75 enrolled • 3 to 20 months post-MI • Total-C < 240; LDL-C between 115 and 174; Triglycerides < 350 mg/dL • 5 yr Treatment with Pravastatin 40 mg vs. placebo Sacks, F. et al, N Engl J Med 1996; 335:1001-9
CARE - Study Endpoints • Primary: • CHD death or nonfatal MI • Secondary: • CHD death • Tertiary: • Total Mortality • Others: • Fatal MI, nonfatal MI, PTCA, CABG, Stroke Sacks, F. et al, N Engl J Med 1996; 335:1001-9
CARE - Baseline Characteristics • 86% male; 14% female • Mean age 59 ± 9 years • 93% white • 21% current smoker • 42% hypertensive • 14% diabetic Sacks, F. et al, N Engl J Med 1996; 335:1001-9
CARE - Baseline Characteristics • Mean 10 ± 5 months post-MI • 54% had prior PTCA / CABG • 83% taking aspirin • 41% taking b-blockers • 40% taking calcium antagonists • 15% taking ACEIs Sacks, F. et al, N Engl J Med 1996; 335:1001-9
Lipids at Baseline Plasma Lipid Placebo Pravastatin (n=2078) (n=2081) Cholesterol (mg/dL) Total 209 209 VLDL 27 27 LDL 139 139 HDL 39 39 Triglycerides (mg/dL) 155 156 Sacks, F. et al, N Engl J Med 1996; 335:1001-9
Percent LDL Reduction on Treatment P < 0.001 for all comparisons Sacks, F. et al, N Engl J Med 1996; 335:1001-9
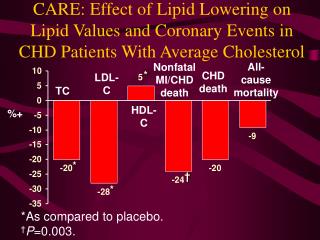
Fatal CHD or Nonfatal Myocardial Infarction (Primary Endpoint) 24% Risk Reduction p = 0.003 Sacks, F. et al, N Engl J Med 1996; 335:1001-9
Coronary Bypass Surgery or Angioplasty 27% Risk Reduction p<0.001 Sacks, F. et al, N Engl J Med 1996; 335:1001-9
CARE - Achievement of Endpoints • Primary: CHD death or nonfatal MI • 24% reduction p = 0.003 • Secondary: CHD death • 20% trend to reduction p = 0.10 (ns) • Tertiary: Total Mortality • 9% trend to reduction p = 0.37 (ns) Sacks, F. et al, N Engl J Med 1996; 335:1001-9
CABG/PTCA/Combined 26% reduction (p=0.005) PTCA 23% reduction (p=0.01) Combined CABG/PTCA 27% risk reduction (p<0.001) Other: Stroke 31% reduction (p=0.03) CARE - Achievement of Endpoints • Fatal MI • 37% reduction (p=0.07) • Nonfatal MI • 23% reduction (p=0.02) • Combined MI endpoints • 25% reduction (p=0.002) Sacks, F. et al, N Engl J Med 1996; 335:1001-9
CARE - Observations • Fatal CHD + nonfatal MI + CABG + PTCA • Women vs. Men: 46% vs. 20% • Current smokers vs. other: 33% vs. 22% • < 60 yr vs. > 60 yr: 20% vs. 27% • EF < 40% vs. > 40%: 28% vs. 23% • Hypertension, yes vs. no: 23% vs. 24% • Diabetes, yes vs. no: 25% vs. 23% • Prior PTCA/CABG, yes vs. no: 22% vs. 25% p values for all subgroups were statistically significant Sacks, F. et al, N Engl J Med 1996; 335:1001-9
CARE - Observations • Baseline LDL influence on Events* • LDL 125-150 26% p < 0.001 • LDL < 125 3% p = 0.85 • LDL > 150-175 p = 0.008 *Events included; fatal CHD, nonfatal MI, CABG or Angioplasty Sacks, F. et al, N Engl J Med 1996; 335:1001-9
CARE - Safety • No difference in fatal and nonfatal primary cancers ... except • Breast Cancer: • Placebo (n=1) • Pravastatin (n=12), p=0.002* Of the 12 breast cancer cases in the pravastatin group, all were nonfatal; 3 occurred in patients who had previously had breast cancer, 1 was ductal carcinoma in situ, and 1 occurred in a patient who took pravastatin for only six weeks. Sacks, F. et al, N Engl J Med 1996; 335:1001-9
Summary Cholesterol lowering with pravastatin in patients with MI and TC < 240 mg/dL Reduced Fatal CHD or nonfatal MI 24% Fatal MI 37% Nonfatal MI 23% All MI, fatal or nonfatal 25% Coronary artery bypass surgery 26% Coronary angioplasty 23% Stroke 31% Sacks, F. et al, N Engl J Med 1996; 335:1001-9
Expected Number of Cardiovascular Events Preventable by Treating 1000 Patients with Pravastatin for Five Years Number of Events Events Total Group Age > 60 Women Fatal CHD 11 27 10 Nonfatal Ml 26 46 83 CABG 25 32 34 PTCA 37 20 66 Strokes TIA 13 25 28 Other Cardiovascular 38 57 7 All Cardiovascular Events 150 207 228 Patients with 1 event pre- 51 71 97 vented Sacks, F. et al, N Engl J Med 1996; 335:1001-9
Conclusion • These results demonstrate that the benefit of cholesterol-lowering therapy extends to the majority of patients with coronary disease who have average cholesterol levels Sacks, F. et al, N Engl J Med 1996; 335:1001-9