Download
1 / 29
300 likes | 612 Views
LATE PERCUTANEOUS CORONARY INTERVENTION AFTER MYOCARDIAL INFARCTION: A META-ANALYSIS. Presenter: Darryn L. Appleton, MBChB Coauthors: Antonio Abbate, MD, Giuseppe GL Biondi-Zoccai, MD, Venkat Ramachandran, MD, Michael J. Lipinski, MD, Pierfrancesco Agostoni, MD, George W Vetrovec, MD.

E N D
LATE PERCUTANEOUS CORONARY INTERVENTION AFTER MYOCARDIAL INFARCTION: A META-ANALYSIS Presenter: Darryn L. Appleton, MBChB Coauthors: Antonio Abbate, MD, Giuseppe GL Biondi-Zoccai, MD, Venkat Ramachandran, MD, Michael J. Lipinski, MD, Pierfrancesco Agostoni, MD, George W Vetrovec, MD
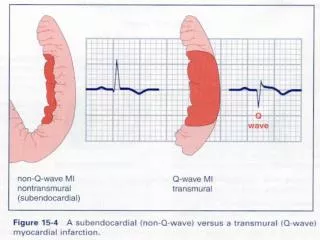
Background • Late presentation with acute STEMI a relatively common and challenging problem • Clear evidence supporting efficacy of primary PCI early in acute STEMI (within 12hrs) • Utility of PCI late in the course of STEMI in otherwise stable patients (>12hrs) has not been proven
Late Open-Artery Hypothesis • Late patency of the IRA correlates closely with improved survival after acute MI • Observational studies (retrospective) have shown improved outcomes in patients with patent IRA vs permanent occlusion • Experimental data in lab animals shows increased apoptosis and adverse remodeling with permanent coronary occlusion
Clinical Question & Objectives • Clinical Question: Does mechanical intervention (PCI) to achieve reperfusion of the IRA late in the course of acute MI (>12hrs from symptom onset) translate to clinical benefit? • Hypothesis: That PCI late in acute MI improves survival by means of reduced adverse remodeling and improved cardiac function • Objectives: to perform a meta-analysis of all relevant trials testing the above hypothesis
Methods • Databases: Pubmed, PubMed Central and mRCT • Search updated Sept 06 (and later March 07) • Search terms: • ‘randomized’, ‘percutaneous coronary intervention’, ‘PCI’, ‘stent’, ‘angioplasty’, ‘revasc*’, ‘recanaliz*’, ‘acute myocardial infarction’, ‘AMI’, ‘infarct*’, ‘occlusion’, ‘occlu*’(where * denotes a wildcard) • Inclusion criteria for trials: • Random treatment allocation • Comparison of PCI to optimal medical management • Randomized >12 hrs following onset of proven acute myocardial infarction • Hemodynamically stable patients that would not need and urgent cardiac cathetization for other indications such as post-infarction angina or inducible ischemia
Methods • Data collection • Pre-specified forms used to collect data on baseline characteristics and outcomes • Statistical methods • performed using Review Manager 4.2.4 • binary outcomes combined with Peto fixed effect model • continuous variables compared using fixed effect inverse variance weighting method • formal Cochran Q chi-square tests performed to investigate heterogeneity between trials • reported values were two-tailed and results were considered statistically significant at the 0.05 level.
Methods • Primary outcome: Death from all causes • Secondary outcomes: • Composite endpoint of death, recurrent MI or hospitalization for CHF • Change in Left-ventricular EF • Cardiac remodeling: changes in ESV and EDV
Total (95% CI) 601 592 100.00 0.49 [0.30, 0.81] Total events: 22 (PCI), 43 (Medical Rx) Test for heterogeneity: Chi² = 5.09, df = 6 (P = 0.53), I² = 0% Test for overall effect: Z = 2.80 (P = 0.005) Results: Primary outcome Outcome: Death from all causes Study PCI Medical Rx Peto OR Weight Peto OR or sub-category n/N n/N 95% CI % 95% CI Year TOPS 0/42 0/45 Not estimable 1992 TOMIIS 1/25 1/19 3.14 0.75 [0.04, 12.76] 1994 Horie 1/44 5/39 9.20 0.21 [0.04, 1.11] 1998 TOAT 2/32 1/34 4.76 2.12 [0.21, 21.13] 2002 Zeymer et al 6/149 17/151 34.92 0.36 [0.15, 0.84] 2003 DECOPI 8/109 9/103 25.73 0.83 [0.31, 2.23] 2004 BRAVE-2 4/182 8/183 19.07 0.51 [0.16, 1.60] 2005 Silva et al 0/18 2/18 3.18 0.13 [0.01, 2.12] 2005 0.1 0.2 0.5 1 2 5 10 Favours PCI Favours medical Rx
Results: Secondary outcomes Outcome: Composite of death, non-fatal MI, hospitalization for CHF Study PCI Medical Rx Peto OR Weight Peto OR or sub-category n/N n/N 95% CI % 95% CI Year TOPS 2/42 3/45 4.18 0.71 [0.12, 4.26] 1992 TOMIIS 1/25 1/19 1.68 0.75 [0.04, 12.76] 1994 Horie 4/44 12/39 11.42 0.25 [0.09, 0.75] 1998 TOAT 9/32 8/34 11.23 1.27 [0.42, 3.79] 2002 Zeymer et al 9/149 24/151 25.85 0.37 [0.18, 0.76] 2003 DECOPI 14/109 16/103 22.68 0.80 [0.37, 1.73] 2004 BRAVE-2 13/182 12/183 20.48 1.10 [0.49, 2.47] 2005 Silva et al 0/18 3/18 2.48 0.12 [0.01, 1.23] 2005 Total (95% CI) 100.00 0.61 [0.42, 0.88] Total events: 52 (PCI), 79 (Medical Rx) Test for heterogeneity: Chi² = 10.56, df = 7 (P = 0.16), I² = 33.7% Test for overall effect: Z = 2.63 (P = 0.008) 0.1 0.2 0.5 1 2 5 10 Favours PCI Favours medical Rx
TOPS 2.0000 (1.1800) 18.00 2.00 [-0.31, 4.31] 1992 TOMIIS 1.2000 (1.5100) 13.28 1.20 [-1.76, 4.16] 1994 Horie 2.8000 (1.2100) 17.50 2.80 [0.43, 5.17] 1998 DECOPI 5.0000 (0.8500) 24.61 5.00 [3.33, 6.67] 2004 Silva et al 4.2400 (1.9100) 9.45 4.24 [0.50, 7.98] 2005 Results: Secondary outcomes Outcome: Change in LVEF Study EF change % (random) Weight EF change % (random) or sub-category EF change % (SE) 95% CI % 95% CI Year Total (95% CI) 100.00 3.17 [1.65, 4.68] Test for heterogeneity: Chi² = 7.51, df = 4 (P = 0.11), I² = 46.7% Test for overall effect: Z = 4.1 (P < 0.0001) 10 5 0 -5 -10 Favours Medical Rx Favours PCI
Results: Impact of OAT & TOSCA-2 studies • NIH funded OAT study published Dec 2006 in NEJM • 2166 patients 3-28 days following acute STEMI, randomized to PCI or optimal medical management, followed for mean of 3 years • TOSCA-2 is a subgroup of the patients randomized in the OAT who had additional baseline and follow-up EF measurements
Results: Impact of OAT study Outcome: Death from all causes Study PCI Medical Rx Peto OR Peto OR or sub-category n/N n/N 95% CI 95% CI Year Dzavik et al (1994) 1/25 1/19 0.75 [0.04, 12.76] 1994 OAT (2006) 87/1082 84/1084 1.04 [0.76, 1.42] 2006 Ellis et al 0/42 0/45 Not estimable 1992 Hochman et al 2/32 1/34 2.12 [0.21, 21.13] 2002 Horie et al 1/44 5/39 0.21 [0.04, 1.11] 1998 Schoemig et al 4/182 8/183 0.51 [0.16, 1.60] 2005 Silva et al 0/18 2/18 0.13 [0.01, 2.12] 2005 Steg et al 8/109 9/103 0.83 [0.31, 2.23] 2004 Zeymer et al 6/149 17/151 0.36 [0.15, 0.84] 2003 Total (95% CI) 1683 1676 0.84 [0.65, 1.10] Total events: 109 (PCI), 127 (Medical Rx) Test for heterogeneity: Chi² = 11.38, df = 7 (P = 0.12), I² = 38.5% Test for overall effect: Z = 1.26 (P = 0.21) 0.1 0.2 0.5 1 2 5 10 Favours PCI Favours medical Rx
Results: Impact of OAT study Outcome: Composite of death, non-fatal MI, hospitalization for CHF Study PCI Medical Rx Peto OR Peto OR or sub-category n/N n/N 95% CI 95% CI Year Dzavik et al (1994) 1/25 1/19 0.75 [0.04, 12.76] 1994 OAT (2006) 173/1082 153/1084 1.16 [0.91, 1.47] 2006 Ellis et al 2/42 3/45 0.71 [0.12, 4.26] 1992 Hochman et al 9/32 8/34 1.27 [0.42, 3.79] 2002 Horie et al 0.25 [0.09, 0.75] 1998 4/44 12/39 Schoemig et al 13/182 12/183 1.10 [0.49, 2.47] 2005 Silva et al 0/18 3/18 0.12 [0.01, 1.23] 2005 Steg et al 14/109 16/103 0.80 [0.37, 1.73] 2004 Zeymer et al 9/149 24/151 0.37 [0.18, 0.76] 2003 Total (95% CI) 1683 1676 0.96 [0.79, 1.17] Total events: 225 (PCI), 232 (Medical Rx) Test for heterogeneity: Chi² = 18.82, df = 8 (P = 0.02), I² = 57.5% Test for overall effect: Z = 0.39 (P = 0.69) 0.1 0.2 0.5 1 2 5 10 Favours PCI Favours medical Rx
Results: Impact of OAT Outcome: Change in LVEF Study EF change % (random) EF change % (random) or sub-category EF change % (SE) 95% CI 95% CI Year Dzavik et al (1994) 1.2000 (1.5100) 1.20 [-1.76, 4.16] 1994 TOSCA-2 (2006) 0.8000 (0.4500) 0.80 [-0.08, 1.68] 2006 Ellis et al -1.0000 (0.8600) -1.00 [-2.69, 0.69] 1992 Horie et al 3.8000 (0.7600) 3.80 [2.31, 5.29] 1998 Silva et al 4.2400 (1.9100) 4.24 [0.50, 7.98] 2005 Steg et al 5.0000 (0.8500) 5.00 [3.33, 6.67] 2004 Total (95% CI) 2.25 [0.30, 4.19] Test for heterogeneity: Chi² = 38.41, df = 5 (P < 0.00001), I² = 87.0% Test for overall effect: Z = 2.26 (P = 0.02) 10 5 0 -5 -10 Favours PCI Favours Medical Rx
Results: Impact of OAT Outcomes: Changes in EDV and ESV Study EDVI change (random) EDVI change (random) or sub-category EDVI change (SE) 95% CI 95% CI Year Horie et al -8.7000 (2.0000) -8.70 [-12.62, -4.78] 1998 Silva et al -5.2000 (2.5700) -5.20 [-10.24, -0.16] 2005 TOSCA-2 (OAT) 2006 -2.1000 (1.1100) -2.10 [-4.28, 0.08] 2006 Total (95% CI) -5.10 [-9.44, -0.77] Test for heterogeneity: Chi² = 8.64, df = 2 (P = 0.01), I² = 76.9% Test for overall effect: Z = 2.31 (P = 0.02) -10 -5 0 5 10 Favours PCI Favours medical Rx Study ESVI change (random) ESVI change (random) or sub-category ESVI change (SE) 95% CI 95% CI Year Horie et al -7.3000 (1.7900) -7.30 [-10.81, -3.79] 1998 Silva et al -6.4000 (2.2900) -6.40 [-10.89, -1.91] 2005 TOSCA-2 (OAT) 2006 -2.7000 (1.6900) -2.70 [-6.01, 0.61] 2006 Total (95% CI) -5.33 [-8.32, -2.35] Test for heterogeneity: Chi² = 3.84, df = 2 (P = 0.15), I² = 47.9% Test for overall effect: Z = 3.50 (P = 0.0005) -10 -5 0 5 10 Favours PCI Favours medical Rx
Limitations • Conflicting results for clinical end-points before and after addition OAT trial data • Inherent limitations of individual studies within meta-analysis impact on overall result • Possible small study selection bias • Wide range of publication dates • Significant improvements in the medical management of acute MI over time • Change in PCI technology itself over time • Some important differences in study design • Lack of apparent statistical heterogeneity • Important to note some key methodologic differences • Pre-treatment with thrombolytics • Inclusion of patients with total IRA occlusion vs “significant stenosis” • Variable length of follow-up
Conclusions • Regarding PCI in stable survivors of acute STEMI, current data including the recent OAT shows that late (> 12hrs) PCI is neithersuperiornor inferior to optimal medical therapy alone in terms of altering survival, or any other combined clinical endpoint
Conclusions • Change in EF and measurements of EDV and ESV show statistically significant improvement with PCI beyond medical therapy alone • Discrepancy between lack of clinical benefit and apparent improvement in EF raises interesting questions: • Is the difference in the change in EF a real phenomenon, and if so, is it large enough to be clinically relevant? • Are benefits of reduction in adverse cardiac remodeling and improved EF offset by late adverse events?
Acknowledgements • A special thanks to Dr George Vetrovec and the VCU Pauley Heart Center Department of Cardiology
Discussion • Areas of ongoing uncertainty • Patients with contraindications to important medications considered standard of care post-MI, e.g. beta-blockers, statins, ACE inhibitors • Subgroups of patients may preferentially benefit from revascularization in the setting of late MI • Patients with more severe LV dysfunction e.g. < 30% • Patients presenting between 12-72 hours • Patients with demonstrable myocardial viability
Results: Secondary outcomes(sensitivity analysis including TOAT) Outcome: Change in LVEF Study EF change % (random) Weight EF change % (random) or sub-category EF change % (SE) 95% CI % 95% CI Year TOPS 2.0000 (1.1800) 18.00 2.00 [-0.31, 4.31] 1992 TOMIIS 1.2000 (1.5100) 13.28 1.20 [-1.76, 4.16] 1994 Horie 2.8000 (1.2100) 17.50 2.80 [0.43, 5.17] 1998 TOAT 2.0000 (1.2300) 17.17 2.00 [-0.41, 4.41] 2002 DECOPI 5.0000 (0.8500) 24.61 5.00 [3.33, 6.67] 2004 Silva et al 4.2400 (1.9100) 9.45 4.24 [0.50, 7.98] 2005 Total (95% CI) 100.00 2.98 [1.67, 4.30] Test for heterogeneity: Chi² = 8.63, df = 5 (P = 0.12), I² = 42.1% Test for overall effect: Z = 4.45 (P < 0.00001) 10 5 0 -5 -10 Favours Medical Rx Favours PCI
For further slides on these topics please feel free to visit the metcardio.org website:http://www.metcardio.org/slides.html