Download
1 / 51
510 likes | 727 Views
Treatment of DVT/PE (VTE) Update 2010 L. Bernardo Menajovsky, MD, MS. Case Study. Message #1. Waiting is NOT Acceptable!. “It is inappropriate to wait for symptoms and then rely upon the diagnosis and treatment of established VTE”. Chest. 2004 and 2008. Consequences of VTE. Recurrent VTE

E N D
Treatment of DVT/PE (VTE)Update 2010L. Bernardo Menajovsky, MD, MS.
Waiting is NOT Acceptable! “It is inappropriate to wait for symptoms and then rely upon the diagnosis and treatment of established VTE” Chest. 2004 and 2008
Consequences of VTE • Recurrent VTE • Post-thrombotic syndrome (PTS)1 • Presence of leg symptoms (pain, cramps, heaviness, pruritus, and paresthesia) and signs (pretibial edema, skin induration, hyperpigmentation, new venous ectasia, redness and pain during calf compression) • Mortality2 1. Prandoni P et al. Haematologica. 1997;82:423-428. 2. Pengo V et al. N Engl J Med. 2004;350:2257-2264.
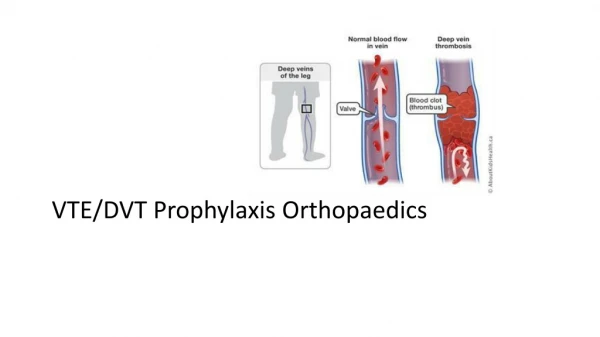
Abnormal Blood Flow Abnormal Vessel Wall Abnormal Blood The Hypercoagulable State (thrombophilia) Dr. Rudolph Virchow 1821-1902
Facts • 50% clinically significant DVT – Asymptomatic • 60-70% of Fatal PE – Asymptomatic DVT Heit JA, et al. Arch Intern Med. 1999;159:445.
The Challenge of Assessing Venous Thromboembolism Symptomatic VTE Silent DVT/PE Decieving
Therapeutic Goals and Treatment Options for DVT Goals of Supportive IVC Heparin LMWH Thrombolysis Therapy Care Filter ? Prevent Embolization Prevent Extension Reduce Recurrence Restore Patency ? Prevent Post-thrombotic Syndrome
ATIII Ternary complex ATIII ATIII ATIII Fixed Variable Pentasaccharide sequence LMWH HEPARIN
Factor Xa Inactivation: LMWH/Heparin Xa ATIII Pentasaccharide sequence Xa ATIII
Thrombin Inactivation: LMWH&Heparin Heparin/ATIII/IIa Ternary complex accelerates inactivation of IIa by ATIII IIa Pentasaccharide sequence IIa AT AT Pentasaccharide sequence LMW Heparin/ATIII No acceleration of inactivation of IIa by ATIII without ternary complex
Authors Leizorovicz et al ‘94 Lensing et al ‘95 Siragusa et al ‘96 Gould et al ‘99 Dolovich et al ’00 van den Belt ‘00 Outcomes More or as effective < Major bleeding < Thrombocytopenia Treatment DVT LMWH Vs UFH Meta-analyses
UFH • Therapeutic levels -- First 24 hours. • Otherwise, risk of recurrent VTE -- 15 X Hull, et al. NEJM 1986; 315, 1109-13 Brandjes DPM et al. NEJM 1992; 327, 1485-90
Advantages of LMWHs • Pharmacokinetics • Reduced protein binding • Predictable dose • Longer plasma half- life • Smaller molecule • Less platelet effect • Clinical Advantage • Better bioavailability • No monitoring • QD or Q12hr dosing • Better SC absorption • Less Thrombocytopenia
Concerns With LMWH Use • Obesity • Renal insufficiency • Pregnancy • Adverse effects • osteoporosis • HIT HIT = heparin-induced thrombocytopenia
Recommendations: Weight Factor • Actual Body Weight Dose up to 155 kg • Unfractionated Heparin for morbid obesity • Select Target Weight Ceiling • Choose a range but obtain Anti-Xa levels to evaluate dose
UFH • Therapeutic levels -- First 24 hours. • Otherwise, risk of recurrent VTE -- 15 X • Caution in obese patients: • aPTT not reliable • Higher risk of bleeding • Heparin resistance Hull, et al. NEJM 1986; 315, 1109-13 Brandjes DPM et al. NEJM 1992; 327, 1485-90 Chest 2004
Heparin Resistance 40 K IU total daily dose = mononuclear white cell = acute phase proteins (histidine-rich glycoprotein, vitronectin, and PF-4) = heparin = vascular endothelial cell
Dosing Issues • What dose should be administered to patients with renal insufficiency? • Do patients with renal insufficiency have increased risk for bleeding? • How about obese patients?
Vitamin K Utilization Reduced Warfarin Mechanism of Action Vitamin K VII IX X II Synthesis of Dysfunctional Coagulation Factors Warfarin
Warfarin: Dosing Information • Individualize dose according to patient response(as indicated by INR) • Use of large loading dose not recommended* • May increase hemorrhagic complications • Does not offer more rapid protection • Low initiation doses are recommended for elderly/frail/liver-diseased/malnourished patients • Adequate overlap! *Harrison L, et al. Ann Intern Med 1997;126,133-136.
FDA Approves Updated Warfarin (Coumadin) Prescribing InformationAugust 16, 2007 • One-third of patients receiving warfarin metabolize it quite differently than expected. Research has shown that some of the unexpected response to warfarin depends on a patient's variants of the genes CYP2C9 and VKORC1. • "Although genetic testing can currently identify who has these genetic variants, more studies are needed to explore the precise starting dose for these patients,"
General Aspects • Short-term treatment associated with 15-50% frequency of extension of thrombus or recurrent disease. • Minimum duration 3 months. • Treatment with VKA is the preferred approach for long-term treatment.
6 – 12 months vs. Indefinite 3 months Indefinite Menajovsky L.B. Am J Med in press
Bleeding Risk factors • >75 yo. • Previous GI bleeding (especially not reversible cause) • Chronic renal or hepatic disease • Concomitant Anti-platelet therapy • Serious or acute illness • Poor anticoagulation control • Suboptimal anticoagulation monitoring
Caval Interruption • Contraindication or complication of Anticoagulation • Recurrent Thromboembolism despite adequate anticoagulation • Massive PE: hemodinamically unstable • Chronic recurrent embolism with pulmonary hypertension • Concurrent pulmonary embolectomy or endarterectomy Sixth ACCP Consensus Conference Chest 2001; 119:176S-193S
IVC Filters • ComplicationsReported Rates (%) Death 0.12 • Recurrent PE 0.5–6 • IVC Occlusion 2–30 • Filter Embolization 2–5 • Access Site Thrombosis 0–6 • Migration* 0-18 • IVC Penetration* 0-41 • Filter Fracture 2-10 • * Clinically significant migration/IVC penetration is rare
New Anticoagulants ORAL PARENTERAL TF/VIIa TFPI (tifacogin) TTP889 X IX APC (drotrecogin alfa) sTM (ART-123) RivaroxabanApixaban LY517717 YM150 DU-176b Betrixaban TAK 442 IXa VIIIa Va AT Xa FondaparinuxIdraparinux II DX-9065a IIa Dabigatran Fibrinogen Fibrin Adapted from Weitz & Bates, J Thromb Haemost 2007
Direct Thrombin inhibition Tissue factor XIIa XIa VIIa IXa Xa II × Factor IIa(thrombin) Dabigatran
Direct Factor Xa inhibition XIIa Tissue factor × XIa VIIa IXa Xa Rivaroxaban Apixaban YM150 DU-176b LY517717 Betrixaban TAK 442 Factor II(prothrombin) Fibrinogen Fibrin clot