Download

1 / 80
820 likes | 1.09k Views
THROMBOPHILIA DVT PROPHYLAXIS VTE MANAGEMENT. DR. ASHISH Moderator: DR. MEERA KHARBANDA. www.anaesthesia.co.in anaesthesia.co.in@gmail.com. Thrombophilia. Thrombophilia - propensity for thrombotic events

E N D
THROMBOPHILIA DVT PROPHYLAXIS VTE MANAGEMENT DR. ASHISH Moderator: DR. MEERA KHARBANDA www.anaesthesia.co.inanaesthesia.co.in@gmail.com
Thrombophilia Thrombophilia - propensity for thrombotic events Most often manifests clinically in form of venous thrombosis (frequently DVT of lower extremity) Thrombophilia may result from inherited or acquired conditions
Heritable cause of thrombophilia • Decreased anti thrombotic proteins Hereditary antithrombin deficiency Hereditary protein c deficiency Hereditary protein s deficiency
Heritable cause of thrombophilia • Due to increased prothrombotic proteins Factor V Leiden genetic polymorphism Prothrombin G20210A genetic polymorphism
Acquired causes of thrombophilia • Myeloproliferative disorders • Malignancies • Pregnancy & OCP use • Nephrotic syndrome patients • Antiphospholipid antibodies
Hypercoagulable States and Risk for Perioperative Thrombosis High Risk Heparin-induced thrombocytopenia (HIT) Antithrombin deficiency Protein C deficiency Protein S deficiency Antiphospholipid antibody syndrome
Hypercoagulable States and Risk for Perioperative Thrombosis Moderate risk Factor V Leiden genetic polymorphism Prothrombin G20210A genetic polymorphism Hyperhomocysteinemia Dysfibrinogenemia Postoperative prothrombotic state Malignancy Immobilization
Random screening of asymptomatic patients for thrombotic risk has not proved cost effective or clinically efficacious Careful history focusing on prior thrombotic events, family H/O thrombosis, & concurrent drug therapy offers greater predictive value than random screening.
Common Inherited Thrombotic Disorders Factor V Leiden(=activated protein C resistance) Point mutation of factor V gene • Results in impaired inactivation of factor V by activated protein C • Factor V leiden stays active in circulation > N , fostering increased thrombin generation • Heterozygosity: 5x ~ 7x risk of VTE Homozygosity: 80x risk of VTE
Prothrombin gene G20210A mutation • Prothrombin gene mutation: nucleotide position 20210: G A • Elevated prothrombin levels and activity • Increased risk of venous thrombosis • Rare in Asians & Africans
Protein C deficiency • Synthesis in the liver; Vit-K dependent • Inactivate factorⅤ and factorⅧ. • It needs a cofactor: protein S • Protein C def. l/t overabundance of thrombin • Risk of thrombosis if warfarin therapy started in absence of protective anticoagulation by heparin
Protein S deficiency • Synthesis in hepatocytes & megakaryocytes • Vit-K dependent • Cofactor of activated protein C(APC) • Protein C have shorter half life than Protein S
Antithrombin Ⅲ deficiency Antithrombin (AT, also called AT III) – defense against clot formation in healthy vessels or at the perimeter of a site of active bleeding Autosomal dominant trait Heterozygosity: 20x risk of VTE Homozygosity: Not compatible with life
In absence of coexisting precipitating conditions, absolute thrombotic risk secondary to heritable thrombophilia proves limited. In the presence of family history or test abnormality suggesting thrombophilia with noh/o thrombosis, risks a/w long-term preventive anticoagulation may outweigh potential benefits.
After a thrombotic complication, however, these patients most often are managed with life-long anticoagulation.
Acquired thrombophilia- Antiphospholipid Syndrome • Autoimmune disorder ch/by venous and/or arterial thromboses , recurrent pregnancy loss. • 20 to autoimmune disorders such as SLE or RA, or occur in isolation. • Mild prolongation of aPTT & + testing for lupus anticoagulant or anticardiolipin antibodies.
Acquired thrombophilia- Antiphospholipid Syndrome • No increased bleeding risk but risk of thrombosis. • Isolated prolongation of an aPTT in preoperative patient consider - antiphospholipid syndrome. • Risk of recurrent thrombosis - life-long anticoagulation.
HIT • Autoimmune-mediated drug reaction - 5% of pt. receiving heparin therapy. • Heparin – AT complex also binds to platelet factor 4 & some pt. develop - • Heparin- induced ab. that can cross react with this platelet binding site to produce platelet clumping and subsequent thrombocytopenia • Can be triggered by low dose heparin as well as therapeutic – dose heparin
MALIGNANCY • Adenocarcinomas of pancreas, colon, stomach, & ovaries . • Pathogenesis - release of procoagulant factor(s) by tumor, which directly activate factor X, endothelial damage by tumor invasion, and blood stasis. • Lab: No abnormalities or some combination of thrombocytosis, elevation of the fibrinogen level, and low-grade DIC.
Pregnancy and OCP Use • Incidence - 1 in 1500 pregnancies • Risk of PE highest during 3rd trimester & immediate postpartum period • Antithrombin III–deficient women high risk -anticoagulated throughout pregnancy. • Factor V Leiden and the prothrombin G20201A mutation a/w less risk. • Women with one of these inherited traits not anticoagulated unless – h/o PE or recurrent DVT
Pregnancy and OCP Use • Since low-dose estrogen OCP introduction -incidence decreased. • Women - smoke, h/o migraine headaches, inherited hypercoagulable defect at increased risk (30-fold) of venous thrombosis, PE, & cerebrovascular thrombosis.
Nephrotic Syndrome Patients • Risk of thromboembolic disease including renal vein thrombosis. • D/t < N levels of antithrombin III or PC 20 renal loss of coagulation protein, factor XII deficiency, platelet hyperactivity, abnormal fibrinolytic activity, & > N levels of other coagulation factors. • Hyperlipidemia and hypoalbuminemia - also possible etiologic factors
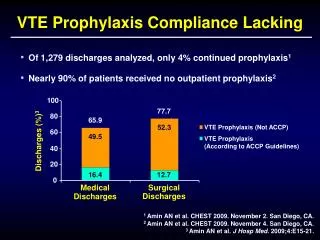
Perioperative venous thromboembolism • Without prophylaxis, incidence of DVT 14% in gynaecological surgery 22% in neurosurgery, 26% in abdominal surgery, 45–60% in orthopaedic surgery.
Agency for health care research and quality have issued report stating that : Prophylaxis for venous thromboembolism is single most important measure for ensuring patient safety in hospitalized patients
Patients at risk for VTE • Surgery : major surgery: abdominal , gynecologic,urologic, orthopedic, neurosurgery, cancer related surgery • Trauma : multisystem trauma, spinal cord injury, spinal #, # of hip and pelvis • Malignancy : any malignanacy, risk higher during chemo & radiotherapy • Acute medical illness: stroke, acute MI, heart failure,neuromuscular weakness syndrome(GBS)
Patients at risk for VTE • Patient specific risk factor: H/o VTE, Obesity, increasing age > 40yr, hypercoagulable state( estrogen therapy) • ICU related factors: prolonged mechanical ventilation, neuromuscular paralysis(drug induced), CVC, severe sepsis, consumptive coagulopathy, HIT
Risk assessment model (RAM) from the ACCP Low risk • Uncomplicated minor surgery in patients <40 yr with no clinical risk factors Minor surgery: performed under local anesthesia or spinal anesthesia last < 30 min
Risk assessment model (RAM) from the ACCP Moderate risk factor • Major and minor surgery in pt. 40–60 yr with no clinical risk factors • Major surgery in pt. <40 yr with no additional risk factors • Minor surgery in pt. with risk factors Major surgery : performed under GA and last > 30 min Other risk factor : cancer , obesity, h/o VTE, estrogen t/t , hypercoagulable state
Risk assessment model (RAM) from the ACCP High risk • Major surgery in patients >40 yr who have additional risk factors Major surgery : performed under GA and last > 30 min Other risk factor : cancer , obesity, h/o VTE, estrogen t/t, hypercoagulable state
Risk assessment model (RAM) from the ACCP Very high risk • Major surgery in pt. >40 yr plus previous VTE or malignant disease or hypercoagulable state • Elective major orthopaedic surgery or hip # or stroke or spinal cord injury or multiple trauma
Prophylaxis regimens • LDUH1- Unfractionated heparin 5000 u s.c every 12 hr • LDUH2- Unfractionated heparin 5000 u s.c every 8 hr • LMWH1:Enoxaparin 40 mg s.c O.D or Dalteparin 2500 u s.c O.D • LMWH2 :Enoxaparin 30 mg s.c every 12 hr or Dalteparin 5000 u s.c O.D • Mechanical aid: Graded compression stockings or intermittent pneumatic compression
Thrombprophylaxis for hip & knee Sx. • Procedures : Elective hip & knee arthroplasty, hip # surgery Drug regimen: Use any one of following • LMWH:Enoxaparin 30 mg s.c every12hr.Give 1st dose 12-24hr before Sx. Or 6hr after Sx. • Fondaparinaux : 2.5mg s.c O.D .First dose 6-8hr after Sx. • Adjusted dose warfarin to achieve INR of 2-3. Give first dose the evening before Sx.
Thrombprophylaxis for hip & knee Sx. Duration of thromboprophylaxis • For elective hip & knee surgery, prophylaxis should continue for 10 days after surgery B. For hip # surgery , prophylaxis should continue for 28 to 35 days after surgery
Prophylaxis regimens • LDUH1- Unfractionated heparin 5000 u s.c every 12 hr • LDUH2- Unfractionated heparin 5000 u s.c every 8 hr • LMWH1:Enoxaparin 40 mg s.c O.D or Dalteparin 2500 u s.c O.D • LMWH2 :Enoxaparin 30 mg s.c every 12 hr or Dalteparin 5000 u s.c O.D • Leg compression methods: Graded compression stockings(GCS) or intermittent pneumatic compression(IPC)
Methods of thromboprophylaxis • Mechanical - External leg compression • Graded compression stockings • Intermittent pneumatic compression • Pharmacologic • Low dose unfractionated heparin • Low molecular weight heparin • Adjusted dose warfarin • Fondaparinaux
Graded compression stockings Thromboembolic deterrent (TED stockings) • Create 18 mm Hg external pressure at ankles & 8 mm Hg in thigh • Resulting 10 mm Hg pressure gradient – driving force for venous outflow from legs • Shown to reduce VTE when used alone for abdominal & neurosurgery • However considered least effective method – not used alone for moderate & high risk of VTE.
Intermittent pneumatic compression • Inflatable bladders that are wrapped around lower leg • Inflated – create 35 mmHg external compression at ankles & 20 mmHg at thighs • Create pumping action by inflating & deflating at regular interval- augments venous outflow • Used after intracranial Sx & trauma victims who are at risk of bleeding
Low – dose unfractionated heparin Rationale for low dose heparin • Heparin indirect acting drug • Must bind to cofactor anti-thrombinIII(AT) to produce effect • Heparin-AT complex inactivates factors IIa(thrombin), IXa, Xa, Xia & XIIa • Inactivation of IIa is sensitive Rn occur at heparin doses far below those needed for inactivation of other coagulation factors • Small doses of heparin can inhibit thrombus formation without producing full anticoagulation
Low – dose unfractionated heparin • Dosing regimen: 5000 u b.d or t.d.s daily • More frequent dosing (t.d.s) recommended for higher risk condition • Surgical prophylaxis: 1st dose 2hr before Sx. • Postoperative prophylaxis continued for 7-10 days or untill pt. fully ambulating • Effective thromboprophylaxis for high risk medical cond. & most non-orthopedic surgical prophylaxis
Low molecular weight heparin • More potent & more uniform anticoagulant activity than UFH. • Advantage : Less frequent dosing,lower risk of bleeding & HIT • No need for routine anticoagulant monitoring with full anticoagulant dosing • Disadvantage : 10 times more costly (per day) than UFH • More effective than UFH for orthopedic procedures involving knee & hip, major trauma including spinal cord injury
Low molecular weight heparin • Dose : Enoxaparin O.D. 40 mg for moderate risk cond. & B.D. 30 mg for high risk cond. • Dalteparin O.D. dose 2500 U for moderate risk cond. & 5000 U for high risk cond. • Timing : Non orthopedic Sx. 2 hr before Sx Orthopedic Sx. 6 hr after Sx • Excreted primarily by kidney. • Pt. in renal failure:Enoxaparin dose reduced to 40 mg o.d for high risk cond. • No dose adjustment for Dalteparin
Adjusted dose warfarin Vitamin K antagonist prevents carboxylation activation of coagulation factors II, VII, IX, and X Advantage : • Preop dose not increase bleeding tendency during Sx d/t delayed onset • Can be continued after discharge if prolonged prophylaxis Disadv.: • Multiple drug interactions • Monitoring lab test • Difficulty adjusting doses d/t delayed onset
Adjusted dose warfarin Dosing regimen • Initial dose : 10mg P.O. evening before Sx • F/b 2.5 mg daily starting the evening after Sx. • Dose adjusted keep INR 2-3
Fondaparinux • Synthetic anticoagulant, an anti-Xa pentasaccharide • Predictable anticoagulant effect • No lab. monitoring required. • Prophylactic dose 2.5 mg O.D s.c. inj. given 6-8 hr after Sx. Contraindication : • Severe renal impairment creatinine clearance < 30ml/hr. • Wt. < 50 kg – marked increase in bleeding
Natural course of thromboembolism • DVT in lower extremity may arise in calf vein or in proximal veins • Thrombous may extend proximally to iliac veins & IVC • Incidence of thrombosis in upper extremity increasing d/t widespread use of central venous catheter • DVT may occur in deep pelvic vein or renal vein • Can be thrombous formation in right side of heart d/t atrial fibrillation
Most clinically important & fatal pulmonary embolism occurs from proximal than distal DVT in leg PE occur in 50% of pt. with proximal DVT, while asymptomatic thrombosis of leg vein is observed in 70% pt with PE On early ambulation, thrombus in deep veins may resolve completely