
PURPOSE
L5-S1 interlaminar endoscopic approach for downward migrated L4-5 disc herniated patients with motor weakness. Department of Neurosurgery, Hurisarang spine hospital, Deajeon Woo-jin Choi, M.D., Ki-hyen Jun, M.D., Kwan-tae Kim, M.D. e-mail: neurocwj@dreamwiz.com Mobile : 017-622-8822.

PURPOSE
E N D
Presentation Transcript
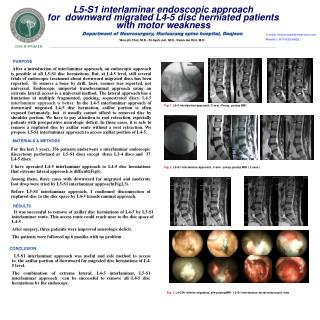
L5-S1 interlaminar endoscopic approach for downward migrated L4-5 disc herniated patients with motor weakness Department of Neurosurgery, Hurisarang spine hospital, Deajeon Woo-jin Choi, M.D., Ki-hyen Jun, M.D., Kwan-tae Kim, M.D. e-mail: neurocwj@dreamwiz.com Mobile : 017-622-8822 ’2008 춘계학술대회 PURPOSE After a introduction of interlaminar approach, an endoscopic approach is possible at all L5-S1 disc herniations. But, at L4-5 level, still several trials of endoscopic treatment about downward migrated discs has been reported. To remove a bone by drill, laser, raemer was reported, not universal. Endoscopic uniportal transforaminal approach using an extreme lateral access is a universal method. The lateral approach has a limitation at multiple fragmented, packing, sequestrated discs. L4-5 interlaminar approach is better. In the L4-5 interlaminar approach of downward migrated L4-5 disc herniation, axillar portion is often exposed fortunately. but it usually cannot offord to removed disc by shoulder portion. We have to pay attention to root retraction, especially patients with preoperative neurologic deficit. In these cases, it is safe to remove a ruptured disc by axillar route without a root retraction. We propose L5-S1 interlaminar approach to access axillar portion of L4-5. Fig. 1. L4-5 interlaminar approach, C-arm / Preop, postop MRI MATERIALS & METHODS For the last 3 years, 356 patients underwent a interlaminar endoscopic discectomy performed at L5-S1 discs except three L3-4 discs and 37 L4-5 discs. I have operated L4-5 interlaminar approach to L4-5 disc herniations that extreme lateral approach is difficult(Fig1). Among them, three cases with downward far migrated and moderate foot drop were tried by L5-S1 interlaminar approach(Fig2,3). Before L5-S1 interlaminar approach, I confirmed disconnection of ruptured disc to the disc space by L4-5 transforaminal approach. Fig. 2.L5-S1 interlaminar approach, C-arm / preop.postop MRI ( 2 case ) RESULTS It was successful to remove of axillar disc herniations of L4-5 by L5-S1 interlaminar route. This access route could reach near to the disc space of L4-5 . After surgery, three patients were improved neurologic deficit. The patients were followed up 6 months with no problem CONCLUSION L5-S1 interlaminar approach was useful and safe method to access to the axillar portion of downward far migrated disc herniations of L4-5 level. The combination of extreme lateral, L4-5 interlaminar, L5-S1 interlaminar approach can be successful to remove all L4-5 disc herniations by the endoscope. Fig. 3.L4-5 Rt inferior migration, pre-postopMRI / L5-S1 interlaminar serial endoscopic view


















