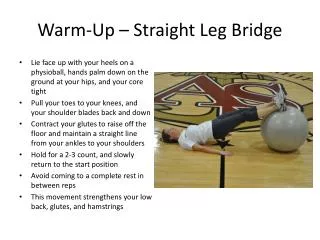
One-arm reach (heels down example)
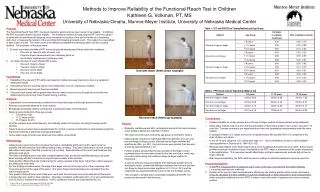
Methods to Improve Reliability of the Functional Reach Test in Children Kathleen G. Volkman, PT, MS University of Nebraska-Omaha, Munroe-Meyer Institute, University of Nebraska Medical Center. Purpose. Table 1: ICC and 95%CI by Testing Method and Age Group.

One-arm reach (heels down example)
E N D
Presentation Transcript
Methods to Improve Reliability of the Functional Reach Test in Children Kathleen G. Volkman, PT, MS University of Nebraska-Omaha, Munroe-Meyer Institute, University of Nebraska Medical Center Purpose Table 1: ICC and 95%CI by Testing Method and Age Group • The Functional Reach Test (FRT) has been studied in adults and has been shown to be reliable.1 In children, the FRT has been shown to be less reliable.2 The traditional method of measuring the FRT is for the subject to stand with the arm flexed 90 degrees and to measure the location of the end of the fist on a measuring stick, then to measure the location of the end of the fist following a forward reach. The subject is not permitted to take a step or to fall. The reach score is the difference between the starting position and the reaching position. The purposes of this study were: • To study test-retest reliability of FRT scores in typically developing children under two conditions: • One-arm vs. two-arm style of reach, and • Finger-to-finger measurement (non-stationary point) vs. • toe-to-finger measurement (stationary point • To study how style of reach affects FRT scores • One-arm, finger-to-finger • Two-arm, finger-to-finger • One-arm, toe-to-finger • Two-arm, toe-to-finger One-arm reach (heels down example) Hypotheses • Reliability of the one-arm FRT will be decreased in children because they tend to be more variable in testing than adults. • Symmetrical two-arm reaching will be more reliable than one-arm reaching in children. • Measuring reach from toes will improve reliability. • One-arm reach scores will be greater than two-arm reach scores across all ages due to the two-arm method placing more body mass forward during reaching. Table 2: FRT Score (cm) by Age Group (Mean ± sd) Subjects • A population of convenience was recruited from a local day camp and through personal contact. • Parental consent was obtained for each subject. • 80 typically developing children participated, including 40 males and 40 females. • Subjects were divided into three age groups. • 7-8 years (n=29) • 11-12 years (n=26) • 15-16 years (n=25) • 69 of the subjects were tested twice for the reliability portion of the study, including 33 males and 36 females. • Subjects were screened using a questionnaire for current or previous orthopedic or neurological symptoms that were treated by a physician or physical therapist. • Active ankle range of motion was observed to be within normal limits Two-arm reach (heels up example) • Conclusions • Highest reliability for all age groups was in the toe-to-finger method of measurement as hypothesized. • Using either method, both one-arm and two-arm styles of reach were similar in ICC values, except in 7-8 year olds. This was contrary to our hypothesis that a two-arm symmetrical measurement would be more reliable. • In younger children, ICC values were lower as hypothesized, with broader 95% CI’s compared to the older children and adults. • In the 15-16 year old group, ICC values were high (.81 - .93) in all methods, similar to adult reliability values published in Duncan et al, 1990 (ICC=.92). • Because start position of the finger was found to move backward during the two-arm reach, there may be another previously unstudied source of variability in the FRT—sway or movement of the center of pressure in the sagittal plane. This movement would affect finger-to-finger measurement methods but not toe-to-finger methods. • With improved reliability, the FRT could be used in children to evaluate treatment outcomes over time. • Recommendations • In the FRT, measuring from a stationary point, such as the toes, may improve test-retest reliability • ( in one-arm and two-arm methods) • Position of the arm for initial measurement is affected by the starting position of the center of pressure. • It may be desirable to instruct children to put their weight back on their heels prior to each measurement (when using the traditional one-arm FRT) in order to move the center of pressure to a more consistent position. • Results • Reliability coefficients and 95% confidence intervals of the four functional reach testing methods are reported in Table 1. • The mean score for each method by age group is reported in Table 2. • Initial analysis revealed no significant difference between one-arm and two-arm finger-to-finger scores, although toe-to-finger methods did significantly differ. (p<.001) One-arm scores were greater than two-arm scores by approximately 6-7 cm. • Further analysis showed that the start position of the finger moved backward when the arms were raised for the two-arm reach, which was not evident when using the traditional finger-to-finger method of measuring. • A second analysis, that accounted for the initial body position prior to starting the reach, showed the difference between the one-arm and two-arm finger-to-finger scores was significant (t=13.15, p<.001) and the magnitude was approximately the same as the toe-to-finger scores. • This revealed a variable which could affect reliability of the FRT not previously discussed in the literature. Methodology • Subjects were given instructions to place their feet a comfortable width apart and to reach as far as possible with their dominant arm without taking a step or falling. They were instructed to choose reaching with either heels down (feet flat) or heels up (up on toes). Demonstration of the reach and these two foot strategies was given. • The lower extremity position was held constant between trials and for the reliability testing by using the same strategy with the feet and by tracing the feet on paper at the first test. • Hand position differed from the traditional test by using a pointed index finger rather than a fist to measure the distal point of the limb. • For toe-to-finger measurements, the edge of the paper was set at the zero point of the measuring stick. Toes were placed at the edge of the paper. The toe-to-finger measurements were calculated from the reach measurement. • One practice trial and three reach trials were used, with the best reach score recorded as the final score. • A single rater was used for data collection. Intraclass correlation coefficients (ICC {1,1}) were estimated for each of the four measurement methods. A 95% confidence interval was estimated for the ICC. • Duncan PW, et al. Journal of Gerontology, 45(6):M192-197,1990. • Donahoe, et al. Pediatric Physical Therapy, 6:189-193,1994.




![[PDF] Free Download Autism in Heels By Jennifer O'Toole](https://cdn4.slideserve.com/8187103/slide1-dt.jpg)