Download
1 / 24
240 likes | 455 Views
HERD PROTECTION BY IMMUNIZATION. W. Paul Glezen, M.D. Herd Protection against Influenza. “…it is apparent that progress in the control of influenza has not been impressive. A reassessment of the basic assumptions upon which the program was developed is warranted.”.

E N D
HERD PROTECTION BY IMMUNIZATION W. Paul Glezen, M.D.
Herd Protection against Influenza “…it is apparent that progress in the control of influenza has not been impressive. A reassessment of the basic assumptions upon which the program was developed is warranted.” A. D. Langmuir et al 1964; Am J Public Health 54:563-71
OBJECTIVES • Recognize the failure of current strategies to control influenza. • Most vulnerable to complications may not respond to vaccine. • High risk persons are not readily accessible for vaccination. • Herd protection by immunization is a well- established concept. • Indirect benefit has been detected for several vaccines. • Several studies have demonstrated herd protection with influenza. • Delivery of influenza vaccine by school and workplace -based clinics • Will improve influenza control. • Will best prepare for the next pandemic.
Problems With TargetingHigh Risk Patients • High risk patients are not easily accessible for vaccination • Many high risk patients are debilitated or immunocompromized and fail to respond optimally to vaccine
Risk Based Strategies Have Failed Universal Recommendations Generally Are More Successful e.g.: > 65 yr, 6-23 mo., Ontario program The most vulnerable persons – elderly and infants – have poor immune responses to vaccines and are at the end of the transmission chain = inefficient use of vaccine.
School Children, Preschool childrenand Working adults have the: • highest attack rates for influenza, • are the spreaders in the community • and the introducers into the household. • They also are most accessible for rapid deployment of vaccine.
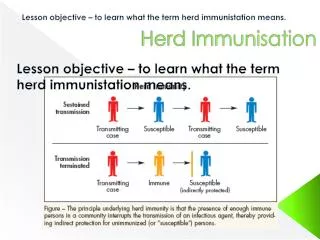
Influenza vaccines generate optimal immune responses in healthy schoolchildrenand working adults. Immunization of these groups has the potential for establishing indirect protection of the vulnerable [HERD IMMUNITY or HERD PROTECTION] = efficient use of influenza vaccine.
Herd Protection by Influenza Vaccines • Tecumseh MI study (Monto et al. Bull WHO 1969;41:537) – 67% reduction in adult illness rates by single dose of TIV in school children. • Northern Territory, Australia (Warburton et al. Med J Aust 1972;2:67) – reduction in attack rate in communities with variable vaccine coverage compared to those with no vaccine. • Novgorod, Russia schoolchildren study (Rudenko et al. J Infect Dis 1993;168:881) – reduction in attack rate in staff where LAIV given to students. • San Diego (Hurwitz et al. JAMA 2000;284:1677) – TIV for daycare toddlers reduced ILI in older siblings and parents. • Moscow, Russia (Ghendon et al. Epidemiol Infect 2006;134:71) TIV in 57% of preschool and 72% of school children reduced illness and complications in unvaccinated, non- institutionalized adults.
Herd protection of elderly by Mass InfluenzaImmunization of Children, Moscow, 2001-2002 Rate Per 1000 Persons Ghendon et al. Epidemiol. Infect 2006;134:71-8.
Clinical Effectiveness of Influenza Vaccine, Moscow, 2001-2002 Direct protection # children #vaccinated %efficacy Kindergarten 6,374 3,659 (57.4%) 60.9 School aged 34,237 24,651 (72%) 68.8 Total 40,611 26,275 (64.7%) 63.7 Indirect (herd) protection Achieved with only 28,310 vaccine doses – sufficient for 34.5% of 82,051 persons > 60 years of age. Ghendon et al. Epidemiol Infect 2006;134:71-8.
Herd Protection – Proof of Concept • In Japan from 1977 to 1987 influenza vaccine was mandatory for school attendance • Two doses of inactivated vaccine/yr • Vaccine not recommended for elderly/high risk • School program reduced influenza-related excess mortality by 35,000 to 47,000 lives/yr Reichert et al. N Engl JMed 2001;344:889
Control of Epidemic Influenza:Study Design • An open-label, non-randomized, community-based trial of annual influenza immunization of school-age children to effect herd immunity.
Control of Epidemic Influenza: Objectives • The primary objective is to determine the proportion of vaccinated school-age children needed to effect herd immunity (indirect effectiveness) against influenza. • The secondary objectives are to assess the direct effectiveness and safety of LAIV. For Direct Effectiveness of LAIV in 2003-2004, see Piedra, et al. Abstract # 726
MAARI Rates in the Intervention and Comparison Sites during Influenza Outbreaksfor SWHP Members > 35 years old Piedra et al: Vaccine 2005;23:1540-8
Piedra et al: Live attenuated intranasal influenza vaccine-trivalent (LAIV-T) administered during the 2003-04 influenza type A(H3N2) outbreak provided immediate, direct and indirect protection in children. PEDIATRICS 2007, in press.
Culture-Positive Medically Attended Acute Respiratory Illness (MAARI) in 5 to 18 Year Old Children, Intervention Site, 2003-04. Never vaccinated 127/231(55%) reference LAIV-T* 19/55(34.5%) 37.3% 0.006 TIV* 14/24(58.3%) 0% NS *LAIV-t = live attenuated influenza vaccine, TIV = inactivated influenza vaccine Vaccine status No.+/No. cultured (%) Efficacy p-value
Proportion of School Children with Influenza-Positive* Cultures by 2-Week Periods, Intervention Site, 2003-04. LAIV-T 10/25(40.0) 4/14(28.6) 5/16(31.3) TIV 7/9(77.8) 7/15(46.7) *A/Fujian(H3N2) Vaccine No. positive/no. cultured (%) by 2-week periods 1-2 3-4 >4
Preliminary Data 2004-2005 Epidemic Caused by Influenza A/California (H3N2) with ~30% Vaccinated with A/Fujian (H3N2) Vaccine. 2005-2006 Epidemic With Emergence of Another New H3N2 Variant, A/Wisconsin (H3N2), plus Influenza B, with ~5,309 received LAIV and 1,904 received TIV containing A/California (H3N2) and B Shanghai/361/2002 (Yamagata lineage) antigens. B outbreak due to B/Ohio, Victoria lineage.
Indirect Effectiveness of School Aged Influenza Vaccine Program on MAARI for Adults > 18 Years of Age, 2004-05 Relative risk of MAARI for Intervention/Comparison Sites at Specified Intervals RR: 0.99 1.00 0.90 1.04 95%CI 0.91,1.07 0.93,1.08 0.84,0.96 0.97,1.11 Pre-epidemic Vaccine delivery Epidemic Post-Epi 18-34 years >35 years RR: 1.04 1.02 0.89 1.06 95%CI 0.99,1.09 0.98,1.07 0.85,0.921.02,1.10
Direct and Indirect Effectiveness of the School-Aged Influenza Vaccine Program during the Influenza B Outbreak, 2005-06, Piedra et al: Pediatric Academic Societies Annual Meeting, May 8, 2007. Relative Risk (RR) for MAARI by Age Group (yr) Epidemic Period <5 5-17 18-34 >35 Pre-epidemic 1.131.20 1.06 1.07 Epidemic 0.96 0.88 0.95 0.94 Underline = significant (95%CI did not cross 1.0)
SUMMARY • LAIV provides almost immediate protection. • A single dose is effective even against most new variants. • 30-40% coverage of schoolchildren prevented the influenza B outbreak of 2005-06. • Protection persists to second season.
CONCLUSIONS 1. Current ACIP recommendations give influenza immunization priority to 218 million people (72.7% of US population) including: a. children 6 – 59 months, b. adults > 50 years, c. high risk 5 – 49 years of age d. pregnant women e. health care workers, caretakers f. household contacts of children < 5 years and all high risk 2. The infrastructure does not exist to accomplish this. 3. A practical complementary strategy is to utilize school-based and workplace-based clinics to systematically immunize all school children and working adults annually.
CONCLUSIONS continued: 4. This would provide time to access elderly and high risk. 5. Viral surveillance must be improved to facilitate efficient use of antivirals. 6. Effective interpandemic control will increase demand for vaccines and antivirals to assure supplies and establish infrastructure for effective utilization of both during the pandemic.