Download
1 / 9
90 likes | 373 Views
Median Nerve Entrapment in a High School Female Softball Player. By Ashlee Capano. History. 15 yr old softball/ clarient player Athlete hurt elbow last softball season prior to entering high school and never received treatment.

E N D
Median Nerve Entrapmentin a High School Female Softball Player By Ashlee Capano
History • 15 yr old softball/clarient player • Athlete hurt elbow last softball season prior to entering high school and never received treatment. • Upon assessment patient reported no mechanism of injury this season but has gotten progressively worse over the past two weeks. • Athlete reported radiculopathy into the third and fourth metacarpals and that her whole arm was cold all the time. • Trouble playing clarinet, typing, and writing. • Athlete reported being awoken by sensations of radiculopathy down the entire arm
Assessment • Inspection revealed no gross deformities, carrying angle discrepencies,bruising, or signs of infection. • Athletes involved arm did appear to be paler than the uninvolved arm with poor capillary refill. • Palpation revealed point tenderness over the medial epicondyle, UCL, and olecranon process. • ROM of the elbow was painful in all planes with strength deficiets in extension, pronation, and flexion. • ROM of the wrist was painful in all planes and there was a decrease in grip strength. • ROM of the shoulder was WNL in all planes. • Dermatome /Myotome assessment revealed dificiencies in c5-c7 patterns.
Assessment Cont’d • None of the MMT were able to be held due to pain • Positive Special Tests • Phallens • Tinel’s Sign • Valgus Stress Test 0/30 for laxity but have a firm end feel. • Delayed C6 reflex
Clinical Impression • Median Nerve Impingement (PronatorTeres Syndrome) with a Grade I UCL sprain • Physician Referral • Imaging
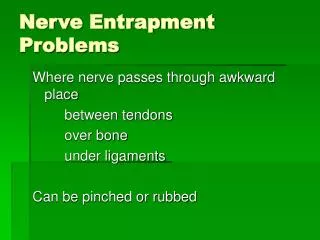
PronatorTeres Syndrome • Similar to carpal tunnel syndrome, pronatorteres syndrome typically squeezes the median nerve producing numbness or tingling in the palm, thumb, forefinger and middle finger • Since the well-known condition of CTS also involves compression of the median nerve, many cases of PTS are mistakenly diagnosed as carpal tunnel syndrome.
Possible Treatment Options • Conservative Treatment: Activity modification to Immobilization for 4-6 weeks depending on severity symptoms • Operative Treatment: Decompression of all four sites of possible pathology
Rehabilitation • ROM- fingers, wrist, elbow, shoulder • Joint Mobilizations • Resistance Exercise • Maintain fitness level • Stretching • Flexibility • Core Strength • Scapular Stabilization