Download
1 / 24
240 likes | 390 Views
HEPATOCELLULAR CARCINOMA Manal Abdel Hamid Associate Prof. Of medical oncology. Epidemiology. Hepatocellular carcinoma is the 5 th most common malignancy worldwide & the 3 rd cause of cancer related death with male-to-female ratio 5:1 in Asia 2:1 in the United States

E N D
HEPATOCELLULAR CARCINOMAManal Abdel HamidAssociate Prof. Of medical oncology
Epidemiology • Hepatocellular carcinoma is the 5th most common malignancy worldwide & the 3rd cause of cancer related death with male-to-female ratio • 5:1 in Asia • 2:1 in the United States • Tumor incidence varies significantly, depending on geographical location. • HCC with age. • 53 years in Asia • 67 years in the United States.
Etiology • Hepatitis B • -increase risk 100 -200 fold • - 90% of HCC are positive for (HBs Ag) • Hepatitis C • Cirrhosis • - 70% of HCC arise on top of cirrhosis • Toxins -Alcohol -Tobacco -Aflatoxins • Autoimmune hepatitis • States of insulin resistance- Overweight in males Diabetes mellitus
Incidence according to etiology Abbreviations: WD, Wilson′s disease; PBC, primary biliary cirrhosis, HH, hereditary hemochromatosis; HBV, hepatitis B virus infection; HCV, hepatitis C virus infection.
Signs & symptoms • Nonspecific symptoms • abdominal pain • Fever, chills • anorexia, weight loss • jaundice • Physical findings • abdominal mass in one third • splenomegaly • ascites • abdominal tenderness
Guidlines (a)which patients are at high risk for the development of HCC and should be offered surveillance (b) what investigations are required to make a definite diagnosis (c) which treatment modality is most appropriate in a given clinical context.
Guidlines (a) which patients are at high risk for the development of HCC & should be offered surveillance - M &F with established cirrhosis due to HBV and/ or HCV, particularly those with ongoing viral replication - M &F with established cirrhosis due to genetic haemochromatosis - M with alcohol related cirrhosis who are abstinent from alcohol or likely to comply with treatment - M with primary biliary cirrhosis Abdominal US and AFP/ 6 months
Diagnosis (b) what investigations are required to make a definite diagnosis • AFP produced by 70% of HCC > 400ng/ml AFP over time 2)Imaging -focal lesion in the liver of a patient with cirrhosis is highly likely to be HCC - Spiral CT of the liver - MRI with contrast enhancement
Diagnosis 3)Biopsy is rarely required for diagnosis in 1–3%. Biopsy of potentially operable lesions should be avoided where possible seeding
Diagnosis Cirrhosis + Mass > 2 cm Normal AFP Raised AFP Confirmrd diagnosis CT, MRI
Diagnosis Cirrhosis + Mass < 2 cm Normal AFP Raised AFP CT, MRI Assess for surgery lesion by exam FNAC or biopsy Confirmed diagnosis
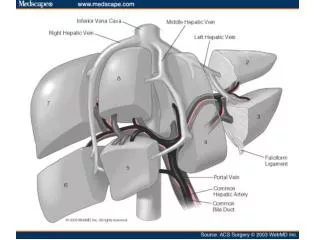
Treatment (Surgery) • The only proven potentially curative therapy for HCC • Hepatic resection or liver transplantation • Patients with single small HCC (≤5 cm) or up to three lesions ≤3 cm • Involvement of large vessels (portal vein, Inferior vena cava) doesnt automatically mitigate against a resection; especially in fibrolamellar histology • No randomised controlled trials comparing the outcome of surgical resection and liver transplantation for HCC.
Treatment (Surgery) • Hepatic resection should be considered in HCC and a non-cirrhotic liver (including fibrolamellar variant) • Resection can be carried out in highly selected patients with cirrhosis and well preserved hepatic function (Child-Pugh A) who are unsuitable for liver transplantation. It carries a high risk of postoperative decompensation. • Perioperative mortality in experienced centres remains between 6% and 20% depending on the extent of the resection and the severity of preoperative liver impairment. • The majority of early mortality is due to liver failure.
Treatment (Surgery) • Recurrence rates of 50–60% after 5 years after resection are usual (intrahepatic) • Liver transplantation should be considered in any patient with cirrhosis • Patients with replicating HBV/ HCV had a worse outlook due to recurrence and were previously not considered candidates for transplantation. • Effective antiviral therapy is now available and patients with small HCC, should be assessed for transplantation
Treatment (non-Surgical) should only be used where surgical therapy is not possible. • Percutaneous ethanol injection (PEI) • has been shown to produce necrosis of small HCC. • It is best suited to peripheral lesions, less than 3 cm in diameter • Radiofrequency ablation(RFA) • High frequency ultrasound to generate heat • good alternative ablative therapy • No survival advantage • Useful for tumor control in patients awaiting liver transplant
Treatment (non-Surgical) 3) Cryotherapy • intraoperatively to ablate small solitary tumors outside a planned resection in patients with bilobar disease 4) Chemoembolisation • Concurrent administration of hepatic arterial chemotherapy (doxirubicin) with embolization of hepatic artery • Produce tumour necrosis in 50% of patients • Effective therapy for pain or bleeding from HCC • Affect survival in highly selected patients with good liver reserve • Complications: (pain, fever and hepatic decompensation)
Treatment (non-Surgical) 5) Systemic chemotherapy • very limited role in the treatment of HCC with poor esponse rate • Best single agent is doxorubicin (RR: 10- 20%) • Combination chemotherapy didn’t response but survival • should only be offered in the context of clinical trials 6) Hormonal therapy • Nolvadex, stilbestrol and flutamide 7) Interferon-alfa 8) retinoids and adaptive immunotherapy (adjuvant)
Targeting angiogenesis for HCC • HCC is one of the most vascular tumor • Major driver of angiogenesis is vascular endothelial growth factor (VEGF) • Sorafenib and bevacezumab target VEGF in HCC • Bevacizumzb: Median OS of approximately 12 months • Bevacizumab + erlotinib: Medain OS 15-17 months
Investigational combination therapies in HCC • Combinations under investigations • Bevacizumzb + erlotinib • Sorafenib +erlotinib • Combination therapy will likely be used to treat HCC in the future
HCC (Whats ahead?) • Combinations therapy • Bevacizumzb or Sorafenib + Erlotinib • Sorafenib + mTOR inhibitor • Early sequential therapies