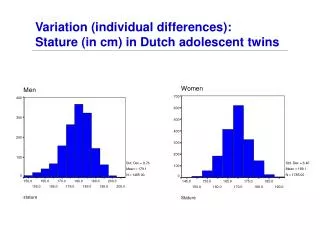
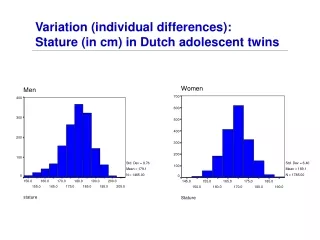
Short stature
Growth Hormone Deficiency 生长激素缺乏症 Xue Fan Gu, MD, PhD Xinhua Hospital Shanghai Jiao Tong University School of Medicine. Short stature. Below the 3rd percentile or - 2SD than that of his or her peers

Short stature
E N D
Presentation Transcript
Growth Hormone Deficiency生长激素缺乏症Xue Fan Gu, MD, PhDXinhua HospitalShanghai Jiao Tong University School of Medicine
Short stature • Below the 3rd percentile or -2SD than that of his or her peers • Short stature has many causes, the pathologic short stature should be suspected in children who have an abnormal growth velocity or who are significantly short for their family
Growth Hormone Chemistry:191 animo acid,22-KDa protein Action: • To growth of the epiphyseal regions of the long bones, also via induce local IGF-1 production in the epiphyseal plate at the both level of mRNA and protein. • to promote the cell proliferation. • A variety of metabolic effect, such as Anabolic action on protein metabolic, lipolysis, animo acid transport in diaphragm and heart. • “Diabetogenic” action on large GH dose. • The effects in normal aging and catabolic conditions are under investigation.
Etiology of GH deficiency Genetic forms It can be transmitted as an autosomal recessive, autosomal dominat or X-linked recessive trait. Abnormalities of the genes: GHRH receptor, Pouifi, Prop1, GH1, GH receptor, IGF-1 etc. Acquired forms The GH axis is more susceptible to disruption by acquired conditions that are the other hypothalamic-pituitary axes. Craniopharyngioma, eosinophilic granuloma, tuberculosis, Trauma, radiotherapy for malignancies
Clinical manifestations • Short stature: slow growth in height, • Congenital form: birth length is below the mean, 2-4Sd below the mean by 1 year of age. • Acquired form: normal initially, growth faillure gradually appear and progress • Delayed closure of the epiphyses. • The head is round, the face is short and broad. The neck is short, the voice is high-pitched, the genitals are undeveloped and sexual maturation may be delayed or absent. The scalp hair is fine. • Some with ACTH、TSH、GnRH and ADH deficiency.
Laboratory findings (1) • Definitive diagnosis: GH provocative tests: Insulin 0.05-0.1u/Kg Arginine 0.5g/kg Clonidine 4ug/kg L-dopa 10mg/kg Blood GH test at 0、30、60、90min • Peak level less than 10ug: GH deficiency • The frequency of false-negative response to a single testis approximately 20%
Laboratory findings(2) • Additional measurement: IGF-1,IGFBP-3, TSH,T4,ACTH,LHRH. • X ray : Skeletal maturation show bone age is delayed. • Image examination:Skull study by X ray, CT or MRI to observe the calcification, erosion within or above the sella etc..
Differential diagnosis • Chronically disease • Family short stature • Constitutional growth delay • Intrauterine growth retardation • Chromosomal abnormality:45,XO, 47,XX,+21 • Bone abnormality • Emotional deprivation
Treatment • Treatment should be started as soon as possible to narrow the gap in height between patients and their classmates and to have greatest effect on mature height. • GH replacement:0.1 U/kg/d, it is subcutaneously in six or seven • Therapy should be continuous until near final height is achieved.
Stopping treatment : bone age of greater than 14 yr in girl and greater that 16 yr in boys. Replacement should also be directed at other hormonal deficiencies • TSH deficient subjects: L-T4 • ACTH deficient patients: hydrocortisone • Gonadotropins deficient patients: gonaddal steroids