Understanding the Respiratory System Functions and Divisions
Explore the essential functions and divisions of the respiratory system, from gas exchange to voice production and protection. Learn about the upper and lower respiratory tracts, nasal cavities, pharynx, and larynx in detail.

Understanding the Respiratory System Functions and Divisions
E N D
Presentation Transcript
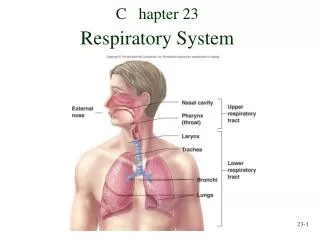
C hapter 23 Respiratory System
Respiration • Ventilation: Movement of air into and out of lungs • External respiration: Gas exchange between air in lungs and blood • Transport of oxygen and carbon dioxide in the blood • Internal respiration: Gas exchange between the blood and tissues
Respiratory System Functions • Gas exchange: Oxygen enters blood and carbon dioxide leaves • Regulation of blood pH: Altered by changing blood carbon dioxide levels (increase C O2 = decrease pH) • Voice production: Movement of air past vocal folds makes sound and speech • Olfaction: Smell occurs when airborne molecules are drawn into nasal cavity • P rotection: Against microorganisms by preventing entry and removing them from respiratory surfaces.
Respiratory System Divisions • Upper tract: nose, pharynx and associated structures • Lo w er tract: larynx, trachea, bronchi, lungs and the tubing within the lungs
Nose (Nasus) and Nasal C avities • External nose (visible part – includes hyaline cartilage plates & nasal bones ) • N asal cavity • From nares (nostrils) to choanae (openings into the pharynx) • Vestibule: just inside nares – lined with stratified squamous epithelium – continuous with skin • Hard palate: floor of nasal cavity – separates nasal cavity from oral cavity – covered by mucous membrane • N asal septum: partition dividing cavity. Anterior cartilage; posterior vomer and perpendicular plate of ethmoid (divides nasal cavity into right & left parts) • C hoanae: bony ridges on lateral walls with meatuses(passageways) between. Openings to paranasal sinuses and to nasolacrimal duct
Functions of Nasal C avity: • Passageway for air(open even if mouth full of food) • C leans the air [vestibule lined with hair & this traps particles / mucous membrane consists of pseudostratified ciliated columnar epithelium with goblet cells (mucus)] • Humidifies( moisture from mucous membranes & from excess tears that drains into nasal cavity through nasolacrimal duct), warms air ( warm blood flowing through mucous membranes - this prevents damage to respiratory passages caused by cold air) • Smell [superior part of nasal cavity consists of olfactory epithelium (sensory receptors)] • Along with paranasal sinuses are resonating chambers for speech
Pharynx: • C ommon opening for digestive and respiratory systems (connected to respiratory at larynx & to digestive at esophagus) • Three regions • N asopharynx: a. Pseudostratified columnar epithelium with goblet cells. b. Mucous and debris from nasal cavity is swallowed. c. Openings of Eustachian (auditory) tubes – air that passes through them to equalize air pressure between atmosphere & middle ear. d. Floor is soft palate (separates nasopharynx from oropharynx), uvula is posterior extension of the soft palate – prevents swallowed materials from entering nasopharynx & nasal cavity • Oropharynx: shared with digestive system (extends from soft palate to epiglottis). Lined with moist stratified squamous epithelium – air, food, & drink passes through. • Laryngopharynx: epiglottis to esophagus. Lined with moist stratified squamous epithelium – food & drink pass through here to esophagus (very little air passes / too much air = gas)
Larynx - base of tongue to trachea / passageway for air • U npaired cartilages • Thyroid: largest, Adam’s apple • C ricoid: most inferior, base of larynx (other cartilages rest here) • Epiglottis: attached to thyroid and has a flap near base of tongue. Elastic rather than hyaline cartilage • Paired • Arytenoids: attached to cricoid • C oniculate: attached to arytenoids • C uneiform: contained in mucous membrane • Ligaments extend from arytenoids to thyroid cartilage • Vestibular folds or false vocal folds • True vocal cords or vocal folds: sound production. Opening between is glottis - laryngitis is an inflammation of mucosal epithelium of vocal folds
Functions of Larynx • Maintain an open passageway for air movement: thyroid and cricoid cartilages • Epiglottis and vestibular folds prevent swallowed material from moving into larynx – during swallowing, epiglottis covers the opening of larynx so, food & liquid slide over epiglottis toward esophagus. Also, closure of vestibular folds can also prevent the passage of air----when person holds breath. • Vocal folds are primary source of sound production. Greater the amplitude of vibration, louder the sound (force of air moving past vocal cords determines amplitude). - Frequency of vibration determines pitch. Also, length of vibrating segments of vocal folds affect-------ex: when only anterior parts of folds vibrate, higher pitched tones are produced & when longer sections of vibrate, lower tones result. - Arytenoid cartilages and skeletal muscles determine length of vocal folds and also abduct the folds when not speaking (only breathing) to pull them out of the way making glottis larger (allows greater movement of air). • The pseudostratified ciliated columnar epithelium (lines larynx)traps debris, preventing their entry into the lower respiratory tract.
Trachea - windpipe • Membranous tube of dense regular connective tissue and smooth muscle; supported by 15-20 hyaline cartilage C-shaped rings (protects & maintains open passageway for air) . Posterior surface is devoid of cartilage & contains elastic ligamentous membrane and bundles of smooth muscle called the trachealis. C ontracts during coughing-----this causes air to move more rapidly through trachea, which helps expel mucus & foreign objects. • Inner lining: pseudostratified ciliated columnar epithelium with goblet cells. Mucus traps debris, cilia push it superiorly toward larynx and pharynx. Divides to form • Left and right primary bronchi (each extends to a lung) • C arina: cartilage at bifurcation (forms ridge). Membrane of carina especially sensitive to irritation and inhaled objects initiate the cough reflex
Tracheobronchial Tree and C onducting Zone • Trachea to terminal bronchioles which is ciliated for removal of debris. • Trachea divides into two primary bronchi. (right is larger in diameter & more in line with trachea than left) • Primary bronchi divide into secondary (lobar) bronchi (one/lobe) which then divide into tertiary (segmental) bronchi. • Bronchopulmonary segments: defined by tertiary bronchi. • Tertiary bronchi further subdivide into smaller and smaller bronchi then into bronchioles (less than 1 mm in diameter), then finally into terminal bronchioles. • C artilage: holds tube system open; smooth muscle controls tube diameter----- ex: during exercise, diameter increases, decreases resistance to airflow, increases volume of air moved during asthma attack, diameter decreases, increases resistance to airflow, decreases volume of air flow • As tubes become smaller, amount of cartilage decreases, amount of smooth muscle increases------ex: terminal bronchioles have no cartilage & only have smooth muscle.
Respiratory Z one: Respiratory Bronchioles to Alveoli • Respiratory z one: site for gas exchange • Respiratory bronchioles branch from terminal bronchioles. Respiratory bronchioles have very few alveoli (small, air filled chambers where gas exchange between air & blood takes place). Give rise to alveolar ducts which have more alveoli. Alveolar ducts end as alveolar sacs that have 2 or 3 alveoli at their terminus. • Tissue surrounding alveoli contains elastic fibers (alveoli expand during inspiration & recoil during expiration) • No cilia, but debris removed by macrophages. Macrophages then move into nearby lymphatics or into terminal bronchioles.
The Respiratory Membrane • Three types of cells in membrane. • Type I pneumocytes. Thin squamous epithelial cells, form 90% of surface of alveolus. Gas exchange. • Type I I pneumocytes. Round to cube-shaped secretory cells. Produce surfactant (makes it easier for alveoli to expand during inspiration). • D ust cells (phagocytes) • Layers of the respiratory membrane • Thin layer of fluid lining the alveolus • Alveolar epithelium (simple squamous epithelium • Basement membrane of the alveolar epithelium • Thin interstitial space • Basement membrane of the capillary endothelium • C apillary endothelium composed of simple squamous epithelium • Tissue surrounding alveoli contains elastic fibers that contribute to recoil.
Lungs • Two lungs: Principal organs of respiration • Base sits on diaphragm, apex at the top, hilus (hilum)on medial surface where bronchi and blood vessels enter the lung. All the structures in hilus called root of the lung. • Right lung: three lobes. Lobes separated by fissures (deep & prominent) • Left lung: Two lobes • Right lung is larger & heavier than left • Divisions • Lobes (supplied by secondary bronchi), each lobe is subdivided into bronchopulmonary segments (supplied by tertiary bronchi and separated from one another by connective tissue partitions), bronchopulmonary segments are subdivided into lobules (supplied by bronchioles and separated by incomplete partitions). • Note: 9 bronchopulmonary segments present in left lung & 10 present right lung • Note: Individual diseased bronchopulmonary segments can be surgically removed, leaving the rest of lung intact, because major blood vessels & bronchi do not cross connective tissue partitions.
Thoracic Wall • Thoracic vertebrae, ribs, costal cartilages, sternum and associated muscles • Thoracic cavity: space enclosed by thoracic wall and diaphragm • Diaphragm separates thoracic cavity from abdominal cavity
Inspiration and Expiration • Inspiration: diaphragm, external intercostals, pectoralis minor, scalenes • D iaphragm: dome-shaped with base of dome attached to inner circumference of inferior thoracic cage. C entral tendon: top of dome which is a flat sheet of connective tissue. • Q uiet inspiration: accounts for 2/3 of increase in size of thoracic volume. Inferior movement of central tendon and flattening of dome. Abdominal muscles relax • Other muscles: elevate ribs and costal cartilages allow lateral rib movement • Expiration: muscles that depress the ribs and sternum: such as the abdominal muscles and internal intercostals. • Q uiet expiration: relaxation of diaphragm and external intercostals with contraction of abdominal muscles • Labored breathing: all inspiratory muscles are active and contract more forcefully. Expiration is rapid
Pleura • P leural cavity surrounds each lung and is formed by the pleural membranes. Filled with pleural fluid. • Visceral pleura: adherent to lung. Simple squamous epithelium, serous. • P arietal pleura: adherent to internal thoracic wall. • Pleural fluid: acts as a lubricant and helps hold the two membranes close together (adhesion). • M ediastinum: central region, contains contents of thoracic cavity except for lungs.
Blood and Lymphatic S upply • Two sources of blood to lungs: Pulmonary & Bronchial • Pulmonary artery brings deoxygenated blood to lungs from right side of heart to be oxygenated in capillary beds that surround the alveoli. Blood leaves via the pulmonary veins and returns to the left side of the heart. • Bronchial arteries provide oxygenated systemic blood to lung tissue. They arise from the aorta & run along the branching bronchi. Part of this now deoxygenated blood exits through the bronchial veins to the azygous (drains chest muscles); part merges with blood of alveolar capillaries and returns to left side of heart. • Blood going to left side of heart via pulmonary veins carries primarily oxygenated blood, but also some deoxygenated blood from the supply of the walls of the conducting and respiratory zone. • Two lymphatic supplies: superficial and deep lymphatic vessels. Exit from hilus • Superficial drain superficial lung tissue and visceral pleura • Deep drain bronchi and associated C .T. • No lymphatics drain alveoli • Phagocytic cells within lungs phagocytize carbon particles & other debris from inspired air & move them to lymphatic vessels • Older people & smokers lungs appear gray to black because accumulation of these particles • C ancer cells from lungs can spread to other parts of body through lymphatic vessels.
Ventilation • Movement of air into and out of lungs • Air moves from area of higher pressure to area of lower pressure (requires a pressure gradient) • If barometric pressure (atmospheric pressure) is greater than alveolar pressure, then air flows into the alveoli. • Boyle’s La w : P = k/V, where P = gas pressure, V = volume, k = constant at a given temperature • If diaphragm contracts, then size of alveoli increases. Remember P is inversely proportionate to V; so as V gets larger (when diaphragm contracts), then P in alveoli gets smaller.
Alveolar Pressure C hanges: (Note: Barometric air pressure is always assigned a value of zero)