Download
1 / 31
350 likes | 495 Views
Antidiabetic medications and heart disease 26th April 2014, Kuwait. Prof. Dr. Oliver Schnell Diabetes Research Group e.V. at the Helmholtz Center Munich, Germany. Diabetes = CAD risk equivalent. Schramm TK et al., Circulation, 2008; 117: 1945.

E N D
Antidiabetic medications and heart disease26th April 2014, Kuwait Prof. Dr. Oliver Schnell Diabetes Research Group e.V.at the Helmholtz Center Munich, Germany
Diabetes = CAD risk equivalent Schramm TK et al., Circulation, 2008; 117: 1945
Diabetes mellitus, fasting glucose, and risk of cause-specific death Estimated future years of life lost owing to diabetes The Emerging Risk Factors Collaboration. NEJM 2011; 364: 829-841
Diabetes mellitus, fasting glucose, and risk of cause-specific death HR for major causes of death, according to baseline levels of fasting glucose The Emerging Risk Factors Collaboration. NEJM 364 (2011) 829-841
The Munich Myocardial Infarction Registry: Reduction of hospital mortality in patients with acute myocardial infarction 25% D p=0.027 ND 20% p=0.01 16% 14% 15% 12% Hospital Mortality 11% Schnell O et al., Diabetes Care 2004 27: 455-460 10% 10% 5% 4% 4% 5% 0% 1999 2001 1999 2001 < 24h 24h
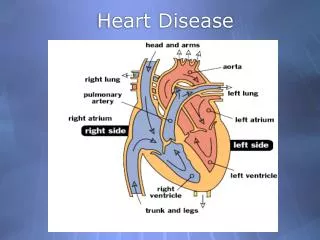
Diabetes and diffuse CHD Right coronary artery Left coronary artery • Female, 58 years • HbA1c: 8.4 % • Duration of diabetes: 15 years • Acute myocardial infarction (MI) • Angiogram: diffuse coronary artery disease
The Munich Myocardial Infarction Registry: CRP-levels and mortality in diabetic and non-diabetic patients * * * * * * * * * * * * * P for trend vs. lowest quintile: * P < 0,05, ** P < 0,01, *** P < 0,001 Otter W, Winter M, Doering W, Standl E, Schnell ODiabetes Care 2007; 30: 3080 - 3082
Impact of diabetes, C-reactive protein and kidney function on hospital mortality in acute myocardial infarction Schnell O et al, Diab Vasc Dis Res 2010; 7: 225-230
The Silent Diabetes StudyExtent of CAD as detected by (a) OGTT Patients without known diagnosis of DM undergoing coronary angiography in relation to severity and (b) HbA1c a.) b.) Doerr R et al. Diabetologia. 2011; 54:2923-30
Hospital mortality and stroke:Diabetic patients vs. non-diabetic patients All patients Diabetic patients Non-diabetic patients Total mortality Mortality ≤ 24 h Braun K, Otter W, Sandor S, Standl E, Schnell O. Diab Res Clin Pract 98 (2012): 164-168
Increase in postprandial blood glucose precedes preprandial blood glucose elevation Breakfast preprandial postprandial Glucose mmol/l Morning Duration of diabetes HbA1c: blue < 6,5 %, red 6,5 – 7 %, green 7,1 – 8 %, orange 8,1 – 9%, brown 9,1 % and higher Monnier L et al, Diabetes Care 2007 (30) 263-269
NAVIGATOR: No effect of nateglinide on prevention of diabetes nor CV outcomes The NAVIGATOR Study Group, NEJM 2010, published online on March 14
1st Co-primary endpoint: MI, Stroke, or CV Death Adj. HR 1.02 (0.94, 1.11) Log Rank P = 0.63 N Engl J Med 2012; 367:319-328
Multifactorial intervention in type 2 diabetes: The Steno 2 study Composite endpoint CV-death, MI or stroke, CABG or PCI, limb amputation or vascular surgery Gaede et al N Engl J Med 2008;358:580-91
Steno 2 Study – 13 year follow up: negative trends in weight management may have challenged the benefits of blood glucose lowering therapy Gaede et al N Engl J Med 2008;358:580-91
ACCORD: Primary Endpoints Subgroups • Evidence of benefit for • Patients without preexisting cardiovascular events • Patients with baseline HbA1c<8% The Action to Control Cardiovascular Risk in Diabetes Study Group, N Engl J Med 2008;358:2545–59
ACCORD VADT ADVANCE Severe Hypoglycemic episodes in ACCORD, VADT, ADVANCE p<0.001 p< 0.01 p<0.001
Mortality and blood glucose in patients with ST elevation MI (n=62) (n=123) (n=280) (n=186) (n=200) (n=196) Glucose levels (mg/dl) Pinto DS, et al. J Am Coll Cardiol 2005;461:178-80.
Effect of experimental hypoglycaemia on QT interval A B QTc 456 ms HR 66 bpm QTc 610 ms HR 61 bpm 5.0 mM 2.5 mM QTc, corrected QT interval from baseline; HR, heart rate Marques et al. Diabet Med 1997;14:648–54
ADA / EASD position statement:Approach to management of hyperglycemia Inzucchi SE et al. Management of hyperglycaemia in type 2 diabetes: a patient-centered approach. Position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia DOI 10.1007/s00125-012-2534-0
Metabolic and cardiovascular effects of GLP-1 Metabolic effects GLP-1 receptor- dependent Cardiovascular effects T1/2= 1-2 min Cardiovascular effects GLP-1 receptor- independent after Drucker DJ. Gastroenterology 2007; 132:2131-2167
GLP-1 Receptors are Present in Cardiovascular Tissues Cardiomyocytes Microvascular endothelium; Coronary smooth muscle Mesenteric artery (medial smooth muscle cells) Endocardium GLP-1-Receptor;green Vascular/cardiac smooth muscle;red Nuclei:blue Ban et al; Circulation 2008
Infarct size is reduced with liraglutide at 28 days post MI in mice Infarct Infarct *p<0.05 vs. placebo 30 * 20 Infarct size (%) 10 0 Liraglutide Placebo Noyan-Ashraf et al. Circulation 2007;116(Suppl)
Initial Combination Therapy With Sitagliptin Plus Metformin Provided Sustained HbA1c Reductions Through 104 Weeks1 APT Population (Extension Study) Sitagliptin 100 mg qd (n=50) Sitagliptin 50 mg bid + metformin 500 mg bid (n=96) Metformin 500 mg bid (n=64) Sitagliptin 50 mg bid + metformin 1000 mg bid (n=105) Metformin 1000 mg bid (n=87) 9.0 24-WeekPhase ContinuationPhase ExtensionStudy 8.5 Mean baseline HbA1c = 8.5%–8.7% LS Mean HbA1c Change From Baseline, % 8.0 –1.1 7.5 –1.2 –1.3 7.0 –1.4 6.5 –1.7 6.0 0 6 12 18 24 30 38 46 54 62 70 78 91 104 Weeks APT=all-patients-treated; bid=twice daily; LS=least-squares; qd=once daily. 1. Williams-Herman D et al. Diabetes Obes Metab. 2010;12(5):442–451.
Sitagliptin vs Glipizide: Weight Change and Incidence of Hypoglycemia1 Sitagliptin + metformin Glipizide + metformin APaT Population(Patients Inadequately Controlled on Metformin) Body weight at week 104 Hypoglycemia over 104 weeks Between-groups difference = –2.3 kg(95% CI: –3.0, –1.6) Between-groups difference = –28.8% (95% CI: –33.0, –24.5) 2,0 0,7 1,5 1,0 0,5 n=253 n=261 LS Mean (±95% CI) Body Weight Change From Baseline, kg Patients With at Least 1 Episode, % 0,0 –0,5 –1,0 –1,5 n=588 n=584 –2,0 –2,5 –1.6 APaT=all-patients-as-treated; CI=confidence interval; LS=least-squares. 1. Seck T et al. Int J Clin Pract. 2010;64(5):562–576.
Sitagliptin vs Glipizide in Patients WithT2DM and End-Stage Renal Disease on Dialysis: HbA1c 54 Weeks1 FAS/LOCF Population Baseline HbA1c; sitagliptin = 7.89%; glipizide = 7.77% 0.0 −0.1 −0.2 −0.3 −0.4 −0.5 Change From Baseline, % −0.6 −0.7 Δ (95% CI) Δ = 0.15% (−0.18, 0.49) −0.8 −0.9 −1.0 0 6 12 18 24 30 36 42 48 54 Week Glipizidea Sitagliptin CI=confidence interval; FAS=full analysis set; LOCF=last observation carried forward. aMean dose of glipizide was 5.3 mg per day. 1. Data on file, MSD.
Dosage of sitagliptin in patients with renal impairment JANUVIA Prescribing information; revised 04/2012http://www.merck.com/product/usa/pi_circulars/j/januvia/januvia_pi.pdf
TECOS: Summary of Study Design1 • Patients aged ≥50 years with T2DM, pre-existing CVD, and: • HbA1c 6.5%–8.0% (48–64 mmol/mol) and dose-stable for ≥3 months on: • Metformin, pioglitazone, or sulfonylurea as monotherapy or any dual combination therapya • OR • Insulin alone or in combination with metformin Sitagliptinb R Placebo Additional oral AHA agents or insulin added according to usual care to target HbA1c goals according to current guidelines (eg, ADA) Continue metformin and/or pioglitazone and/or sulfonylurea, and/or insulin End of Study Visit T M15 T M21 T M27 T M33 T M39 T M45 Visit 1 Randomization (Day 1) V2 M4 V3 M8 AV M12 AV M24 AV M36 AV M48 Brief Visit M18 Brief Visit M30 Brief Visit M42 aMinimum of 2,000 patients on metformin monotherapy. bIf eGFR is ≥50 mL/min/1.73 m2, dose of sitagliptin = 100 mg/d; if eGFR is 30 to <50 mL/min/1.73 m2, dose of sitagliptin = 50 mg/d; if eGFR is <30 mL/min/1.73 m2 during the study, dose reduced to 25 mg/d. TECOS = Trial Evaluating Cardiovascular Outcomes With Sitagliptin; T2DM = type 2 diabetes mellitus; CVD = cardiovascular disease; R = randomization; AHA = antihyperglycemic agent; HbA1c = hemoglobin A1C; ADA = American Diabetes Association; V = visit; M = month;T = telephone contact (study participants will also see their usual-care physician regularly); AV = annual visit; eGFR = estimated glomerular filtration rate. 1. Green JB et al. Am Heart J. 2013;166:983–989.e7.
TECOS: Selected Inclusion and Exclusion Criteria1 TECOS = Trial Evaluating Cardiovascular Outcomes With Sitagliptin; HbA1c = hemoglobin A1C; DPP-4 = dipeptidyl peptidase; GLP-1 = glucagon-like peptide-1; TZD = thiazolidinedione. 1. Green JB et al. Am Heart J. 2013;166:983–989.e7. Inclusion criteria included: • Aged ≥50 years with type 2 diabetes • Documented vascular disease in the coronary, cerebral, or peripheral arteries • Patients with inadequate control (HbA1c of 6.5%–8.0%) for at least 3 months despite: • Stable-dose monotherapy or dual combination therapy with metformin, pioglitazone, and/or a sulfonylurea • Stable dose of insulin as monotherapy or in combination with stable dose of metformin Exclusion criteria included: • Patient has a history of type 1 diabetes mellitus or ketoacidosis • Patient is not able to take sitagliptin • Patient has taken an approved or investigational DPP-4 inhibitor agent, GLP-1 analogue, or a TZD other than pioglitazone within the past 3 months
Anti-hyperglycemic therapy in Type 2 Diabetes Inzucchi SE et al. Management of hyperglycaemia in type 2 diabetes: a patient-centered approach. Position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia DOI 10.1007/s00125-012-2534-0
Recent guidelines emphasize an individualized treatment approach in type 2 diabetes focussing on pts. with vascular complications In diabetic heart disease, treatment strategies, which are not accompanied by hypoglycemia and weight gain are required. DPP-4 inhibition with sitagliptin has shown to be associated with reduction of fasting and postprandial blood glucose reduction of HbA1c As compared to sulfonylureas, sitagliptin provides similar efficacy in reducing HbA1c in patients uncontrolled on metformin, but with no weight gain and fewer reported hypoglycemic episodes Sitagliptin has been shown to be efficacious and well tolerated in patients with insulin therapy or renal impairment The potential for cardiovascular protection is currently being studied in TECOS Take home messages