Esophagus
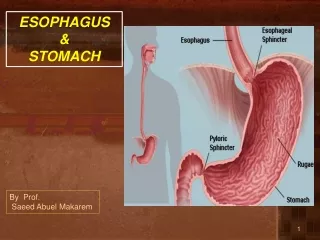
Esophagus. Pimp Session…. The esophagus has no _______. Serosa. It has an inner ____ muscle layer and an outer _____ muscle layer. Circular Longitudinal. Surgical approach to the upper thoracic esoph is via what incision?. Right thoracotomy – avoids the aorta.

Esophagus
E N D
Presentation Transcript
Esophagus Pimp Session…
The esophagus has no _______. Serosa.
It has an inner ____ muscle layer and an outer _____ muscle layer. • Circular • Longitudinal
Surgical approach to the upper thoracic esoph is via what incision? Right thoracotomy – avoids the aorta
Surgical approach to lower thoracic esoph? • Left thoracotomy
Thoracic duct drains into what? • Left subclavian vein
What is the conservative management of a thoracic duct leak? NPO, TPN, give short and medium FAs, avoid long chain FAs. • Short and medium chain fatty acids enter the portal system directly. • Long chain fatty acids enter the lymphatics and travel via the thoracic duct
Abdominal esoph is supplied by what arteries? • Left gastric • Inferior phrenics
The cervical esophagus is supplied by what artery? • Inferior thyroid artery
Normal LES pressure? • 10-20 at rest
Most common site of esoph perforation during EGD? • Cricopharyngeus muscle
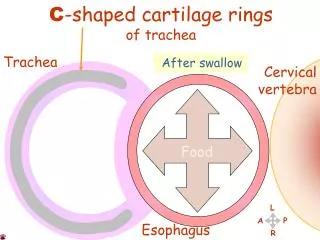
3 anatomic narrowings: • Cricopharyngeus muscle • Compression of L mainstem bronchus and aortic arch • Diaphragm
Aspiration with brainstem stroke is caused by what? • Failure of UES to relax
Procedure of choice to eval dysphagia? • Barium swallow
Plummer Vinson syndrome • Cervical esophageal dysphagia • Cervical esoph web • Fe-def anemia • Treat with dilation and Fe
Treatment of Zenker’s Diverticulum? • Cricopharyngeal myotomy
Achalasia gives you an increase risk of what kind of cancer? • Squamous cell
Achalasia • Dec ganglion cells, Auerbach’s plexus • Aperistalsis, Failure of LES to relax • Bird’s beak on Ba swallow • Tx: lap vs thoracoscopic Heller myotomy
What is the main blood supply to stomach when performing a transhiatal esophagectomy? • Right gastroepiploic artery
What type of cancer is associated with Barrett’s? • Adenocarcinoma
What’s the difference between Mallory Weiss and Boerhaave’s? • Mallory Weiss – esoph tear, usually from retching (not rupture) leads to bleeding. • Boerhaave’s – esoph perf
What do you see on manometry for DES? • Hypertonic, simultaneous contractions
What do you see on manometry for Nutcracker? • Normal peristalsis • High amplitude and duration of contractions.
What do you see on manometry for DES? • Hypertonic, simultaneous contractions
What do you see on manometry for Nutcracker? • Normal peristalsis • High amplitude (>180 mm Hg) and duration of contractions (>6 sec).
What is pseudoachalasia? • Cancer, distal stricture, or tumor of cardia mimicking achalasia.
Alkali esoph: ______ necrosis • Liquefactive necrosis – worse than acid
Acid injury - ______necrosis • Coagulative
How hypertensive is a “hypertensive LES”? • >45 mm Hg
What’s the manometry for “Vigorous” Achalasia? • Partial or absent LES relaxation • And • Repetitive simultaneous contractions (like DES)
What are the indications to operate on paraesophageal hernias? • Ha Ha – trick question!! • Presence of paraesoph hernia is the indication to fix it operatively, for the purpose of the ABSITE.
What esoph leiomyomas get operated on? • >5 cm • Symptomatic
What surgery do you do? • Enucleation
What’s the treatment for high-grade dysplasia? • Esophagectomy • After dx confirmed by 2 pathologists.
Type I-IV hernias? • I – sliding hernia • II – paraesophageal (nml GE junction) • III - combined • IV – colon, spleen or some other organ
Where is a Schatzki’s ring? • Distal esophagus • Assoc with hiatal hernia and GERD • Treat with dilation, may need antireflux procedure.
Where’s a vascular ring? • Abnormality causing a vascular ring external to and compressing the esophagus (or trach)– treat with ligation.
What is the gold-standard test for GERD? • pH probe
What causes epiphrenic diverticula? • Esoph motility disorder • Distal 10 cm of esoph • Treat with diverticulectomy and long esoph myotomy on the opposite side.
Procedure to lengthen esophagus? • Collis gastroplasty
Mechanism of action of omeprazole? • Blocks H/K ATPase
Type I error • Rejects null hypothesis incorrectly • Falsely assume there is a difference when no difference exists.
Type II error: • Accepts null hypothesis incorrectly. • Because of small sample size • Treatments are interpreted as equal when there is actually a difference.
Type III error • Conclusions not supported by data
Null hypothesis: • Hypothesis that no difference exists.
95% Confidence Interval – when is it not statistically significant. • If it includes 1 – it is NOT statistically significant. • The farther from 1 the greater the correlation.